Calcification of the shoulder – What is it and how do we get rid of it?
Feb 2 -
Calcification of the shoulder or calcifying tendinitis is a common cause of limited mobility and shoulder pain. Since calcium plays an important role in our body, it makes sense to understand how calcium can build up in the body (deposits in joints, connective tissue, and vascular walls), which in this case is defined as the pathological condition called calcification.
The most common site of calcium deposition is the joint capsule of the shoulder, i.e. calcification of the shoulder, or the heel, i.e. heel spur.Did you know that calcification of the shoulder often occurs in cycles and that one cycle of calcification formation and breakdown can last up to five years?
Calcification of the shoulder can also be asymptomatic. As many as 43% of patients with shoulder pain have calcifications, and it is more common in women, as 70% of all cases of shoulder calcification involve women. Calcification of the shoulder most often occurs in the 30–50 age group.
Rehabilitation of calcification of the shoulder is complex, and frequent rest and immobility are contraindicated or not recommended, as they usually worsen the condition. For calcification of the shoulder, the first rule of treatment is active physiotherapy with an emphasis on maintaining mobility and strength of the shoulder joint.
Calcifications of the shoulder occur because calcium begins to accumulate in certain areas of the shoulder. Calcification is the body’s protective response to previous injury or overload of soft structures, such as tendons and muscles, but on the other hand, it can also be part of a natural inflammatory reaction to an infection or an autoimmune condition.
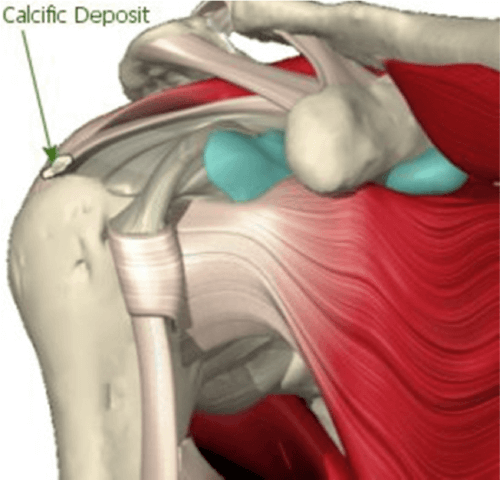
It is typical for the shoulder that calcification begins to form in the area of overloaded tendons, such as the supraspinatus tendon, the infraspinatus tendon, or at attachment sites of other rotator cuff muscles. Calcification is common in individuals who place loads on their arms above head level or compete in sports that involve a lot of repetitive shoulder movement patterns, such as swimming, water polo, volleyball, tennis, and basketball, and often also martial arts.
A characteristic of the formation of calcification of the shoulder is it will begin to occur in the area of tendon microinjury; specifically, because of structural change in the tendon, there will be poorer local blood circulation, and when the injury happens, we often place the shoulder in forced positions and remain still for a long time, which will create conditions for the accumulation of calcium at the site of tendon injury.
Calcification of the shoulder can develop for several years without any noticeable symptoms, but intense pain often appears suddenly. A characteristic of calcifications of the shoulder is that decreased mobility often occurs first, followed by intense pain as the calcium begins to break down. It is typical for calcifications of the shoulder that they start to hurt after a so-called “trigger”, which can be a blow to the shoulder, or even lying on the shoulder for an abnormally long time.
If a calcification of the shoulder is suspected, it is crucial to start treatment in the form of physiotherapy and kinesiology early, as rest, together with movement limitations caused by the calcification of the shoulder, can lead to a frozen shoulder condition, which has a long rehabilitation timeline.
WHEN TO OPT FOR MEDICOFIT DIAGNOSTIC THERAPY?
When shoulder pain lasts longer than one week despite basic measures, it is necessary to undergo diagnostic therapy.
If you notice that you cannot move your arm in all directions as usual, or if mobility is limited due to pain.
If you have had shoulder joint problems before and the symptoms are recurring, it is important to undergo thorough diagnostics.
At MEDICOFIT clinic, we provide patients with calcifications of the shoulder with scientifically supported specialist physiotherapy, which begins with booking a diagnostic therapy appointment.
Two types of calcification can occur in the shoulder: degenerative calcification of the shoulder and reactive calcification of the shoulder.
Degenerative calcification of the shoulder
Degenerative calcification occurs due to age-related microtrauma or chronic overload of the joint capsule, which can also be indirectly caused by weakened rotator cuff muscles. With age, the blood supply of the rotator cuff tendons becomes reduced, and the collagen fibres gradually lose their load-bearing capacity.
Reactive calcification of the shoulder
Reactive calcification of the shoulder is not related to age, but more often occurs as a result of a previous injury, prolonged immobilisation, or a stressful event, and is usually more painful than degenerative calcification of the shoulder. Reactive shoulder calcification has three characteristic phases.
The first phase occurs before the formation of calcification, in the form of pathological changes in the tendon structure that increase the likelihood of calcium crystal formation.
The second phase of reactive calcification of the shoulder is the active calcification phase, where crystal deposits accumulate in the tendon.
In the third phase, the calcification begins to break down, and crystals begin to be released from the tendon into the wider joint space of the shoulder.
Pain most often occurs in the third phase of calcification of the shoulder, when calcium crystals begin to be released from the tendon. A characteristic of the third phase is that it is triggered by a minor traumatic event such as a blow or a quick twist of the arm, a throw, or a fall on the shoulder.
The entire cycle of calcification of the shoulder can last between five and eight years. If the patient does not undergo appropriate conservative treatment in the form of active physiotherapy, calcification of the shoulder lasts longer, with greater movement limitations and more intense pain. If calcification of the shoulder is not treated, frozen shoulder syndrome can develop, with the shoulder becoming practically immobile, and even passive manipulations causing pain.
Risk factors for calcification of the shoulder
Risk factors for developing reactive calcification of the shoulder, which is not caused by age-related changes in connective tissue, are:
hormonal changes (thyroid problems and high levels of oestrogen),
diabetes
incorrect posture (hunched shoulders with thoracic kyphosis and cervical lordosis),
intensive forced shoulder positions (when working at a computer, in dentists, hairdressers, anaesthesiologists, surgeons, painters, and other vocations involving precise work),
prolonged sleeping on one shoulder, excessive strain on the shoulder during sleep,
certain medications,
general lack of exercise (inactive lifestyle),
weakened rotator cuff muscles,
previous rotator cuff muscle or tendon tear,
previous shoulder dislocation,
previous shoulder arthroscopy,
intense, prolonged playing of tennis, basketball, water polo, volleyball.
Diagnosis of calcification of the shoulder
Calcifications of the shoulder are often identified through X-rays, mammograms, etc. The most reliable method for diagnosing calcification of the shoulder is an ultrasound examination (US) of the soft tissues. Ultrasound precisely shows the location of calcification and the degree of degenerative changes in the adjacent connective structures. Ultrasound diagnostics are also used to monitor the progress of treatment of calcification of the shoulder as part of extracorporeal shockwave therapy.If calcification in the shoulder is suspected, MRI diagnostics or magnetic resonance imaging can also be performed, but ultrasound is the most reliable.
Do you have a calcification of your shoulder?
If you have difficulty sleeping at night due to shoulder pain and have difficulty raising your arm above your head, or reaching behind your back with your palm, then it is very likely that you have calcifications in your shoulder. If you also have pain that radiates to the elbow or the entire upper arm, we recommend that you undergo a diagnostic examination of the shoulder, namely an ultrasound scan.
What do you absolutely need to know?
Did you know that the classic physiotherapy approach is often ineffective in the case of calcification of the shoulder? At MEDICOFIT clinic, we treat patients with shoulder mobility limitations on a monthly basis, who have been experiencing severe shoulder pain for several years, but the calcifications have not been eliminated due to the passive physiotherapy approach, which was based on electrotherapy, ultrasound therapy, and mild manual mobilisation.
Below, we present the proper physiotherapy, based on active shoulder mobilisation techniques and extracorporeal shockwave therapy; but before that, let us take a look at the kind of pain calcification of the shoulder causes.
WHY CHOOSE SPECIALIST PHYSIOTHERAPY TREATMENT??
We ensure high treatment success and long-term results.
As much as 95% lower risk of serious complications such as a tendon rupture!
We offer state-of-the-art non-invasive treatment methods that ensure optimal conditions for calcification reabsorption, without surgery.
Comprehensive treatment of calcification of the shoulder at MEDICOFIT clinic is recommended by numerous renowned orthopaedic surgery specialists.
What are the symptoms caused by calcification of the shoulder?
It is characterised by severe pain that limits shoulder mobility, often the arm can only be raised to shoulder height, and reaching higher greatly worsens the pain response – in technical terms, this limitation is called pain-inhibited mobility of the shoulder joint above the head. Calcification of the shoulder often causes night-time pain, characteristically the pain worsens at rest, and sleep may be interrupted or poor.
Typically, the pain of calcification of the shoulder is worse in the lying position than in the standing position. The pain can radiate down the elbow and is also intense in the upper arm, with patients often reporting pain on the entire outside of the arm below the shoulder.
How is calcification of the shoulder treated?
At MEDICOFIT clinic, we provide comprehensive specialised treatment for calcifications of the shoulder, guiding you to a pain-free state with various physiotherapy approaches that are individually tailored to the stage of your calcification of the shoulder.
The leading treatment method for calcification of the shoulder is instrumental physiotherapy with extracorporeal shockwaves (ESWT – extracorporeal shockwave therapy), with simultaneous specialised kinesiology training and active shoulder mobilisation. Comprehensive approach is the only effective approach.
Treatment with physiotherapy and kinesiology is carried out in the third phase of calcification of the shoulder, as the shoulder usually only becomes symptomatic at that time, so we often do not have contact with the patient in the first and second phases of calcification of the shoulder. In the third phase of calcification of the shoulder, the body tries to eliminate the accumulated calcium and begins its reabsorption, which presents in the shoulder as an inflammatory and painful reaction. Due to the accumulation of calcium, limited shoulder mobility can often occur already in the second phase, which becomes even more pronounced due to pain in the third phase, with typical pain particularly at night.
Extracorporeal shockwave therapy
Extracorporeal shockwave therapy uses pulsed action of high-energy waves to break up calcium deposits in the shoulder and accelerate the final, third phase of calcification of the shoulder, facilitating a more effective training approach. Physiotherapy using shockwaves accelerates the division of inflammatory cells and reduces the calcification process. By targeting extracorporeal shockwaves, the cavitation process is triggered, which allows calcifications in soft tissues to be “broken” into smaller fragments and consequently easier reabsorption back into the blood.
Since extracorporeal shockwave therapy is not the most pleasant and can be painful for the patient, the physiotherapist must adjust the intensity of the extracorporeal shockwaves to the patient’s pain threshold and acute symptoms on the day of physiotherapy.
TECAR therapy
For calcifications of the shoulder, we also perform TECAR therapy at MEDICOFIT clinic, which raises the temperature of the connective tissue of the shoulder and enables a greater effect of kinesiology training. TECAR therapy with temperatures reaching 40 degrees Celsius accelerates the breakdown of calcification through the mechanism of calcium dissolution.
Comprehensive treatment of calcification of the shoulder
In addition to extracorporeal shockwave therapy, TECAR therapy, active shoulder mobilisation and special kinesiology training, we also use LASER therapy and HiToP high-tone electrostimulation for calcification of the shoulder, which uses frequencies that are up to 100 times higher than conventional electrostimulation to stimulate cellular metabolism and accelerate the breakdown of calcium. The most effective approach for calcifications of the shoulder is a comprehensive approach that combines extracorporeal shockwaves with various therapeutic techniques. It is crucial for patients to gain adequate rotator cuff muscle strength during shoulder pain rehabilitation.
DANGERS AND PITFALLS OF DELAYED REHABILITATION
MEDICOFIT specialists
Without specialist rehabilitation, calcification can lead to inflammation of the rotator cuff tendons, causing tendon degeneration and even rupture.
Calcium crystals cause inflammation and swelling in the subacromial space, leading to shoulder impingement syndrome.
Long-term limited mobility leads to muscle atrophy and the development of frozen shoulder, which requires several months of rehabilitation.
Inadequate or delayed rehabilitation seriously jeopardises an individual’s long-term physical health and is the main culprit for unsuccessful results and permanent movement limitations.
Is calcification of the shoulder a reason for rest?
Calcification of the shoulder is not a valid reason for rest; on the contrary, rest and lack of movement worsen the pain caused by calcification and cause more severe limitations in shoulder movement. For calcifications of the shoulder, movement is recommended within the range of permissible amplitudes that do not worsen the presenting symptoms, and is performed as part of physiotherapy under the supervision of a kinesiologist. It is crucial for patients to perform strengthening exercises for the kinetic chain of horizontal pulling and pushing with active mobilisation and rotator cuff muscle strengthening exercises throughout their rehabilitation. Strengthening the rotator cuff muscles has been shown to reduce pressure on calcium deposits in the tendons of the shoulder.
The purpose of strengthening exercises is not only to restore range of motion in the joint with calcifications, but also to restore overall shoulder strength and proprioception (the body’s ability to consciously and subconsciously perceive the positions of body parts in space). To gain strength in the shoulder joint, exercises in the initial phase include isometric muscle contraction, which is later upgraded to eccentric/concentric contraction in consultation with a kinesiologist.
When is surgery of calcification of the shoulder recommended?
Approximately 10% of individuals for whom conservative treatment has not helped improve the symptoms of calcification of the should resort to surgery (arthroscopy), primarily due to unbearable pain that only worsens the condition. At MEDICOFIT clinic, we recommend surgical treatment of calcification of the shoulder in rare cases; rehabilitation of calcification of the shoulder without surgery can take several months, even up to 9–12 months.
Unless there has been structured, continuous treatment in the form of comprehensive physiotherapy for at least nine months, we advise against surgical treatment.
Exercises for calcification of the shoulder
Below, we also present some effective exercises that you can incorporate into your routine to reduce discomfort and regain flexibility and strength in your shoulder. Performing these exercises correctly will help you improve your quality of life and prevent further injuries.
Important notice
• The exercise can be performed in numerous modifications and different load regimens; proper execution will be prescribed by a MEDICOFIT physiotherapy specialist for shoulder pain rehabilitation as part of your comprehensive treatment. • If you have shoulder problems, please book an diagnostic therapy appointment before performing the exercise. The exercise may also be contraindicated. • Always do the exercise strictly according to the prescribed regimen and as demonstrated by the physiotherapy specialist for shoulder joint rehabilitation and disorders. • We recommend the exercise as part of guided, comprehensive specialist physiotherapy for shoulder rehabilitation. • If you perform the exercise independently without the supervision of a physiotherapy specialist, we are not responsible for potential symptomatic responses.
Exercise 1: Isometric external rotations + gliding at 60–120° angles of anteflexion
Exercise 2: One-arm external rotations with elastic band + one-arm lateral push
Exercise 3: Shoulder anteflexion through elevation with neutral wrists + elastic band
Book an appointment for shoulder calcification rehabilitation
Department of Medicine. Why is calcium important. University of Wisconsin, School of Medicine and Public Health. Dostopno na: https://www.medicine.wisc.edu/ rheumatology/why-calcium-important.
Health grades. Dostopno na: https://www.healthgrades.com/right-care/vascular-conditions/calcification.
Chianca, Vito, Domenico Albano, Carmelo Messina, Federico Midiri, Giovanni Mauri, Alberto Aliprandi, Michele Catapano, Lorenzo Carlo Pescatori, Cristian Giuseppe Monaco, Salvatore Gitto, Anna Pisani Mainini, Angelo Corazza, Santi Rapisarda, Grazia Pozzi, Antonio Barile, Carlo Masciocchi in Luca Maria Sconfienza. 2018. Rotator cuff calcific tendinopathy: from diagnosis to treatment. Dostopno na: https://pubmed.ncbi.nlm.nih.gov/ 29350647/.
This website uses cookies so that we can provide you with the best user experience possible. Cookie information is stored in your browser and performs functions such as recognising you when you return to our website and helping our team to understand which sections of the website you find most interesting and useful.
Strictly Necessary Cookies
Strictly Necessary Cookie should be enabled at all times so that we can save your preferences for cookie settings.
3rd Party Cookies
This website uses Google Analytics to collect anonymous information such as the number of visitors to the site, and the most popular pages. Keeping this cookie enabled helps us to improve our website.
Please enable Strictly Necessary Cookies first so that we can save your preferences!
Additional Cookies
This website uses the following additional cookies:
(List the cookies that you are using on the website here.)
Please enable Strictly Necessary Cookies first so that we can save your preferences!