Have you ever experienced sudden pain in your shoulder that prevents you from performing the simplest everyday tasks? A rupture of the supraspinatus tendon – one of the most common injuries to the shoulder joint – may be to blame.
Supraspinatus tendon rupture is the most common tendon injury in the body, affecting as many as 30% of people. The incidence under the age of 20 is 9.7%, while in those over the age of 80 it is as high as 62%.
An untreated supraspinatus tendon rupture not only leads to chronic pain but also to serious movement limitations.
Partial or complete rupture or injury to the tendon of the supraspinatus muscle presents as sharp pain and inability to move the arm above head level.
The supraspinatus is one of the four rotator cuff muscles, which are crucial for the stability and mobility of the shoulder joint. Supraspinatus tendon injury most often occurs due to traumatic injury, tendinopathy, or age.
The key to successful rehabilitation is prompt and appropriate treatment. A rupture is primarily treated conservatively in the form of physiotherapy, but in rare cases (large tears), surgical treatment is indicated.
Book an appointment for supraspinatus tendon rupture rehabilitation
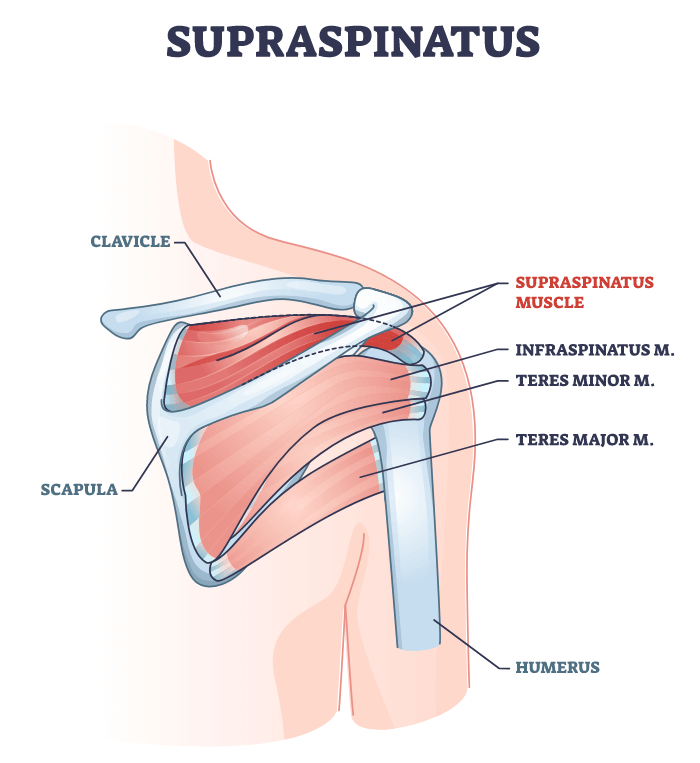
Anatomy of the shoulder joint and the role of the supraspinatus
The shoulder joint is a ball-and-socket joint that is inherently unstable due to its bony structure.
The joint is made up of the head of the humerus and the socket of the scapula (you can imagine this as a large basketball on a shallow plate). The head of the humerus is too large compared to the socket of the scapula, which allows for a large range of motion in the shoulder but consequently has the effect of reduced joint stability.
Stability in the shoulder joint is maintained by static stabilisers (ligaments that stop movement) and dynamic stabilisers (muscles that perform movement).
The main dynamic stabilisers in the shoulder joint are the muscles that make up the rotator cuff and their tendons that wrap around the shoulder joint in all directions.
The rotator cuff is a group of muscles (supraspinatus, infraspinatus, teres minor, and subscapularis) that stabilise the head of the humerus in the socket of the scapula and allow the main movements in the shoulder joint to be performed.
When any of the rotator cuff muscles is injured, there is an imbalance in muscle function and, as a result, reduced stability and mobility in the shoulder joint.
The main function of the supraspinatus muscle is to perform the abduction movement in the first 30 degrees of movement and to stabilise performance of repetitive movements (throwing a ball or making a serve).
Symptoms of supraspinatus tendon rupture
The first signs of a supraspinatus rupture are acute sharp pain, which occurs as a result of a traumatic injury. Initially, the pain is mild, but increases over time and begins to spread to the shoulder area (to the side where the deltoid muscle is anatomically located).
The pain increases with every activity (sports, work, housework) – especially with overhead movements and carrying loads, which over time leads to completely limited function of the individual.

The shoulder joint becomes stiff, which reduces the possible range of motion, with reduced muscle strength (there is an imbalance in the function of the remaining muscles in the shoulder).
Most individuals want to avoid pain with alternative movements, but this affects the function of the entire body’s biomechanics and leads to problems starting to appear elsewhere in the body over time.
Individuals report an inability to sleep on the side where the tendon rupture occurred. Night-time pain limits the quality of sleep.
Causes of supraspinatus tendon rupture
Supraspinatus tendon rupture often occurs due to a traumatic injury that causes microtrauma to the tendon. A microtrauma is an acute injury that ultimately leads to a tendon rupture/tear, as it causes the fibres to deteriorate or degenerate.
Did you know that improper treatment of microtrauma causes ineffective tissue healing, leading to faster degenerative tendon rupture?
Acute tears are more common in the younger population, while degenerative tendon tears are more common in the elderly.
Degenerative tendon rupture is more common in the elderly due to ageing processes that weaken the tendon, which is consequently less susceptible to tensile loads and ruptures more quickly (less external force is required to cause injury).
Supraspinatus muscle injury often occurs due to lifting/carrying too heavy loads, a fall on the shoulder, a sports injury, or a shoulder dislocation.
People over the age of 40, those who perform repetitive shoulder movements (especially difficult and stressful movements), those who work in jobs that involve a lot of movements above shoulder height (painters, plumbers, etc.), or athletes (elite or recreational) are more susceptible to supraspinatus tendon rupture.
WHEN TO OPT FOR MEDICOFIT DIAGNOSTIC THERAPY?
- You have persistent shoulder pain that worsens with movement.
- You are experiencing movement limitations, such as the inability to raise the arm.
- If you have previously had problems with shoulder pain and the symptoms are recurring, this means that the rotator cuff injury was not properly treated.
At MEDICOFIT clinic, we provide patients with scientifically supported specialist physiotherapy, which begins with booking a diagnostic therapy appointment.
Book an appointment for supraspinatus tendon rupture rehabilitation
How is diagnostic therapy done?
The beginning of every physiotherapy treatment is diagnostic therapy, which is performed by a physiotherapist diagnostician and includes:
- anamnesis,
- history of the disease,
- assessment of the arthrokinematics of the shoulder joint and scapula,
- assessment of muscle balance and strength,
- palpation for tenderness,
- sensory tests,
- assessment of pain,
- assessment of grip performance,
- functional movement patterns and
- specific tests.
Here is an example of the questions you will be asked during a diagnostic examination: “How long have you been experiencing pain?” “What movements cause pain?” “Have you had similar problems in the past?”
It is important to make a correct diagnosis of a supraspinatus tendon rupture, as diseases such as SLAP lesion, arthritis, and rotator cuff tendon rupture have similar symptoms.

To confirm the diagnosis, an ultrasound examination (US) is performed, which provides a view of the tendon (which is compared to a healthy shoulder) and a magnetic resonance imaging (MRI) scan, which shows a tear or inflammation of the tendon.
A diagnostic examination is the basis for developing the individualised physiotherapy programme, which is focused on the specific limitations and abilities of each individual.
Book an appointment for supraspinatus tendon rupture rehabilitation
If surgery is indicated, a physiotherapist is crucial in the preoperative and postoperative rehabilitation phase of treatment.
Surgery is not always indicated with a partial rupture of the supraspinatus muscle – in this case, we use physiotherapy treatment.
The primary phase of treatment involves controlling symptoms (inflammation, pain, limited mobility) and promoting healing of diseased tissue with instrumental physiotherapy (HiToP electrotherapy, PERISO diamagnetic therapy, and TECAR therapy).
The next phase of treatment focuses on progressive kinesiology training (first below head level due to limited mobility), which has the effect of increasing muscle strength and mobility in the shoulder (with resistance exercises and mobility exercises).
The specialised kinesiology programme is aimed at establishing appropriate muscle balance and stabilising the entire shoulder girdle and scapulothoracic junction.
Preoperative and postoperative physiotherapy rehabilitation
Surgery is indicated when symptoms persist for a long time and the tear is too large.
The importance of preoperative rehabilitation is in improving muscle strength and mobility, as muscle mass and joint mobility will rapidly decline after surgery.
Postoperative physiotherapy rehabilitation of the shoulder is carried out in accordance with the instructions of the surgeon, who informs the physiotherapist about the technique for suturing the tendon, the size of the tear itself, and the correct range of motion in the shoulder (making sure that there is no recurrence of the rupture).
The short-term and long-term goals of physiotherapy treatment are early stabilisation, muscle strength maintenance and development (with isometric and strengthening exercises), gaining mobility in the joint (Artromot and mobility exercises), and reducing pain (use of instrumental physiotherapy).

The essential guideline of postoperative rehabilitation is to create an appropriate ratio between mobility of the shoulder joint and the scapulothoracic junction and tissue healing.
Postoperative rehabilitation is carried out in the following four phases:
The early phase, lasting up to six weeks after surgery, when the operated arm is in a splint and passive mobility exercises are performed until pain occurs. In the early phase, arm swing exercises and exercises for increasing mobility of other parts of the body are performed. The use of state-of-the-art devices is recommended, such as HiToP electrotherapy to reduce pain and ARTROMOT to increase mobility and prevent stiffness of the shoulder joint.
The middle phase lasts from 6 to 10 weeks, during which active isometric exercises for activating the rotator cuff muscles, exercises for mobility of the shoulder joint and scapulothoracic junction, and active-assisted exercises (assistance with a bar and pulley) begin. Of particular importance in the middle phase are kinesiology exercises for dynamic stabilisation of the shoulder girdle and active exercises for general body strengthening. A physiotherapist begins joint mobilisation during this phase.
The final rehabilitation phase lasts from 10 to 16 weeks, during which active strengthening of dynamic stabilisers (active exercises, resistance exercises) and strengthening of the supraspinatus begin.
The phase of return to normal function begins after 16 weeks, with normal function in the shoulder achieved after 22 weeks or even later. A special kinesiology programme with special exercises (neuromuscular, proprioceptive, etc.) plays an active role in this phase.
DANGERS AND PITFALLS OF DELAYED REHABILITATION

MEDICOFIT specialists
- Without proper rehabilitation, the rupture may enlarge, making treatment more difficult and prolonging recovery time.
- Long-term disuse of the shoulder muscles due to pain and limited mobility causes muscle atrophy, which further weakens the shoulder joint.
- Without appropriate therapy, there is a higher risk of developing adhesive capsulitis, which means significantly limited mobility.
Inadequate or delayed rehabilitation seriously jeopardises an individual’s long-term physical health and is the main culprit for unsuccessful results and permanent movement limitations.
Can supraspinatus tendon rupture be prevented?
A kinesiology programme focused on preventive general strengthening of the body and especially the shoulder girdle prevents tendon rupture. A physiotherapist will provide you with additional advice and demonstrate the correct execution of everyday repetitive movements that cause tensile forces on the tendon.
What do you need to know?
Supraspinatus muscle tear is a common condition that can affect the entire population.
A tear that occurs due to acute causes (traumatic injury, fall, sports injury) more often affects the younger population, while a tear that occurs due to degenerative causes (ageing processes, improperly healed tendon) more often affects the older population.
Vocations involving many repetitive movements that put strain on the arm (such as painters, plumbers, builders, installers) and athletes (involving is a lot of throwing and serving) are more susceptible to rupture of the supraspinatus muscle.
The size of the tear determines what treatment is indicated (conservative – in the form of physiotherapy, or surgical).
In any case, a physiotherapist is indispensable and, using the right methods and procedures, successfully heals the affected tissue and restores function to the arm.
A physiotherapist focuses on improving muscle strength in the arm, improving grip strength, joint mobility, and reducing inflammation.
Successful postoperative rehabilitation takes at least 20 weeks from surgery to full restoration of arm function.
WHY CHOOSE SPECIALIST PHYSIOTHERAPY TREATMENT?
- We ensure high treatment success and guarantee long-term health of the shoulder.
- Reduced risk of shoulder surgery.
- We provide state-of-the-art non-invasive treatment methods that ensure optimal conditions for complete resolution of tendon injuries.
Comprehensive treatment of tendon injuries at MEDICOFIT clinic is recommended by numerous renowned orthopaedic surgery specialists.
Book an appointment for supraspinatus tendon rupture rehabilitation
- May T, Garmel GM. Rotator Cuff Injury. [Updated 2022 Jun 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK547664/
- Sambandam SN, Khanna V, Gul A, Mounasamy V. Rotator cuff tears: An evidence based approach. World J Orthop. 2015 Dec 18;6(11):902-18. doi: 10.5312/wjo.v6.i11.902. PMID: 26716086; PMCID: PMC4686437.
- Kuhta M., 2015. Funkcionalna anatomija in biomehanika ramenskega sklepa. XI. Mariborsko ortopedsko srečanje. Interdisciplinarno strokovno srečanje. Rama v ortopediji. Zbornik predavanj. Maribor, pp. 13-19
- Rečnik G., Mirnik N., Fokter S., 2015. Poškodba rotatorne manšete. Interdisciplinarno strokovno srečanje. Rama v ortopediji. Zbornik predavanj. Maribor, pp. 13-19
- Benazzo, F., Marullo, M. & Pietrobono, L. Supraspinatus rupture at the musculotendinous junction in a young woman. J Orthopaed Traumatol15, 231–234 (2014). https://doi.org/10.1007/s10195-013-0271-x
- Heers G, Anders S, Werther M, et al. [Efficacy of home exercises for symptomatic rotator cuff tears in correlation to the size of the defect]. Sportverletzung Sportschaden : Organ der Gesellschaft fur Orthopadisch-traumatologische Sportmedizin. 2005 Mar;19(1):22-27. DOI: 10.1055/s-2004-813883. PMID: 15776325.
- Akpınar S, Uysal M, Pourbagher MA, et al. Prospective evaluation of the functional and anatomical results of arthroscopic repair in small and medium-sized full-thickness tears of the supraspinatus tendon. Acta Orthopaedica et Traumatologica Turcica. 2011 July-August;45(4):248-253. DOI: 10.3944/aott.2011.2455. PMID: 21908964.
- Tapscott DC, Varacallo M. Supraspinatus Tendonitis. [Updated 2022 Sep 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551702/
- Jo, Y., Kim, W. J., & Lee, H. (2020). Healing of partial tear of the supraspinatus tendon after atelocollagen injection confirmed by MRI: A case report. Medicine, 99(49), e23498. https://doi.org/10.1097/MD.0000000000023498
- Mall, N. A., Lee, A. S., Chahal, J., Sherman, S. L., Romeo, A. A., Verma, N. N., & Cole, B. J. (2013). An evidenced-based examination of the epidemiology and outcomes of traumatic rotator cuff tears. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association, 29(2), 366–376. https://doi.org/10.1016/j.arthro.2012.06.024










