Are you limited by shoulder pain? Did it occur suddenly or have you been experiencing it for a long time? Is it the result of old or new injuries? Are you interested in how modern physiotherapy can help you?
The shoulder joint enables mobility and functionality of the upper extremities, but it is also a place where unpleasant pain can sometimes occur. Shoulder pain is a common problem that can significantly affect our ability to perform everyday activities.
There are many known causes of shoulder pain (traumatic injury, degenerative changes, bone fracture, inflammation of the nerve in the shoulder, inflammation of the shoulder joint), and it is important to identify the main culprit for the pain, as tailored rehabilitation is required depending on the underlying cause!
Our patients often report sharp, dull, or burning pain in the shoulder that spreads into the neck or down the arm, often presenting at night and preventing sleeping on the affected arm.
Did you know that most cases of shoulder pain are successfully treated with physiotherapy treatment? Below we present the main causes of shoulder pain and how they can be successfully treated with specialised physiotherapy.
It is extremely important who you entrust with your body with in the treatment of shoulder pain. Appropriate treatment can only be provided by a team of experts from different fields who cooperate, complement each other, and understand the mechanism of pain and the specifics of your activities.
Because of its anatomical structure, the shoulder joint (glenohumeral joint) is the most mobile joint in the body. It consists of the head of the humerus, the socket of the scapula, and the clavicle.
The size of the head of the humerus compared to the socket of the scapula is disproportionately large, which allows for a large range of motion in the shoulder joint and at the same time causes instability in it.
Stability in the shoulder joint is ensured by muscles that provide dynamic stabilisation and ligaments that provide static stabilisation. Muscles and ligaments keep the head of the humerus in its anatomical position.
The dynamic stabilisers in the shoulder joint are a group of muscles called the “rotator cuff” (subscapularis, infraspinatus, supraspinatus, and teres minor). The combined action of all four rotator cuff muscles ensures muscle balance, which is disrupted in the event of an injury.
The entire shoulder joint is surrounded by a synovial membrane, which is made of fibrous tissue (the outer part) and additionally provides stability and protects the joint.
The inner part of the joint capsule consists of a synovial membrane, which produces synovial fluid, which reduces friction in the joint, maintains optimal sliding in the joint, and contains nutrients for articular cartilage.
Main reasons for shoulder pain
The main reasons for shoulder pain occur because of:
bone fracture,
joint dislocation,
injury or inflammation of the muscle or its tendons,
inflammation of the bursa,
labrum tear,
ligament strain,
compression/inflammation of a nerve in the shoulder,
formation of calcifications, and
wear of articular cartilage.
Through diagnostic therapy, a physiotherapist diagnostician determines the origin of the shoulder pain (on top of the joint, below the joint, in front of the joint, behind or in the joint) and its cause.
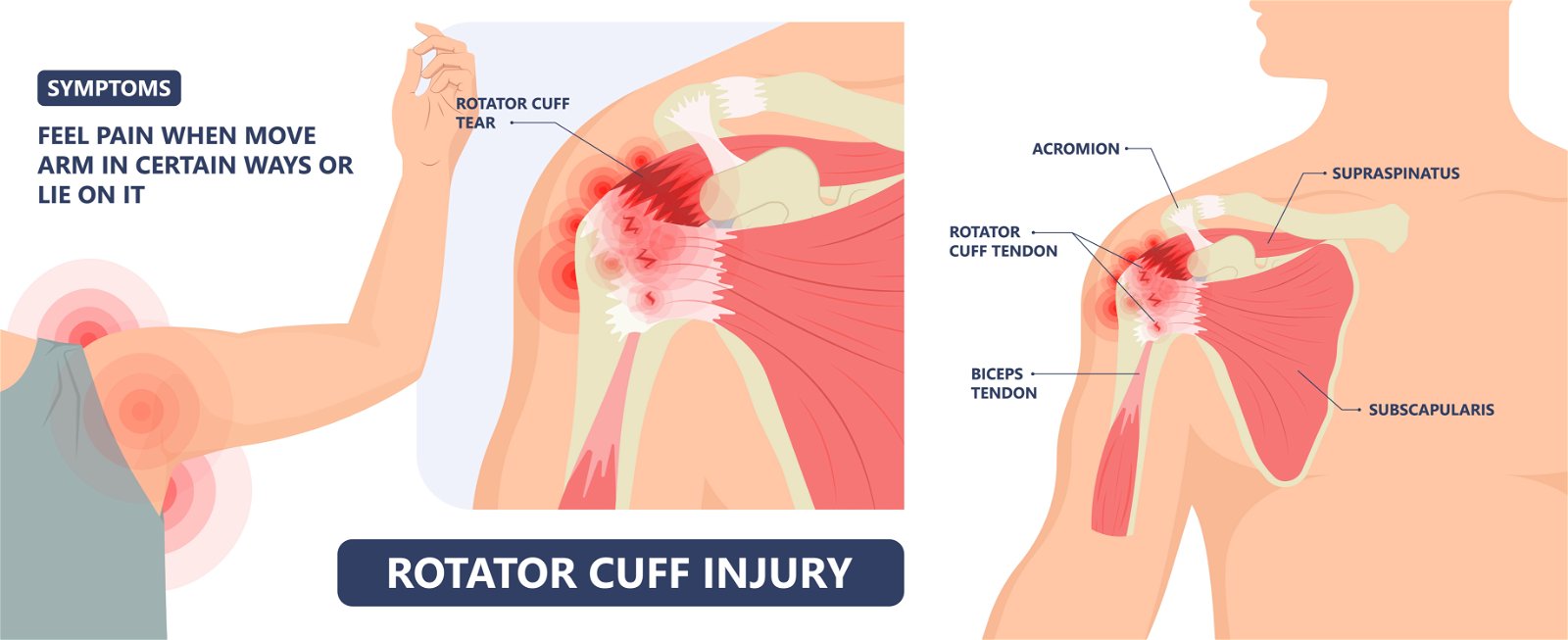
Rotator cuff inflammation or tear
Rotator cuff inflammation or tendinitis occurs due to overload and micro-injuries in the tendon. When pain occurs, there is swelling and tenderness to touch.
A partial or complete tear of the rotator cuff tendon is one of the most common reasons for shoulder pain. A partial or complete tear causes instability in the shoulder joint.
Most often, a tear occurs due to degenerative changes in the body, occasional overload, and micro-injuries to the tissue (traumatic shoulder injury).
Typically, shoulder pain occurs at night (the individual has difficulty falling asleep or wakes up frequently during sleep), during movement (especially with movements above the shoulder joint or when performing throwing movements), the range of motion is limited, and muscle strength rapidly decreases over time.
Individuals report pain in the shoulder outside the joint during a diagnostic examination.
Adhesive capsulitis or frozen shoulder syndrome
Adhesive capsulitis, or frozen shoulder syndrome, is a medical condition that affects the shoulder joint and causes a feeling of stiffness in the joint (resulting in reduced range of motion) and shoulder pain.
A common cause of shoulder pain and stiffness is the thickening and tightening of the joint capsule (fibrous tissue that surrounds and protects the joint). It is currently not known why the joint capsule thickens and tightens.
A typical symptom of frozen shoulder is reduced range of active and passive motion (active motion is when you perform the movement yourself and passive motion is when the movement is performed by a physiotherapist).
Shoulder dislocation and shoulder joint instability
A shoulder dislocation occurs when the head of the humerus bone moves from its original anatomical position and separates from the socket of the shoulder blade. Often times, the ligaments that keep the head in place are damaged.
The most common type of dislocation is anterior dislocation of the shoulder, where there is a high chance of damage to the nerves (causing a burning pain in the shoulder that spreads down the arm) and blood vessels that run under the shoulder joint and supply the entire upper extremity.
It is of utmost importance that the physiotherapist diagnostician checks for correct function of the nervous system and blood circulation during the diagnostic examination.
Did you know that improper treatment of a shoulder dislocation increases the risk of a new dislocation?
Each (new) dislocation increases the chance of instability in the shoulder joint due to chronically damaged ligaments.
SLAP lesion
A SLAP (superior labrum, anterior to posterior) lesion describes damage to the glenoid labrum (the cartilage tissue that surrounds the socket of the shoulder blade).
The name of the injury describes the course of the tear or avulsion (superior labrum, anterior to posterior).
A SLAP lesion is caused by a fall, direct impact, repetitive overuse, and movement. Athletes (volleyball, basketball, track and field) and manual workers (construction, manufacturing workers) are most susceptible to developing a SLAP lesion.
During a diagnostic examination, individuals describe deep pain in the shoulder – more specifically in the front of the shoulder – accompanied by crepitus (a grating sound during movement).
Osteoarthrosis is a common degenerative joint disease that affects not only the knees and hips, but also the shoulder joint. The shoulder joint is crucial for various everyday activities, but age and wear and tear of the joints can lead to shoulder joint arthrosis, causing pain, limitations of mobility, and affecting quality of life.
The main cause of shoulder joint arthrosis is the wear and tear of the cartilage that surrounds the joint surface. With ageing, cartilage naturally wears down, leading to a decrease in its shock-absorbing function and causing friction between the bones.
Did you know that there are other risk factors besides ageing? These are primarily overuse, joint injuries, genetic predisposition, and inflammatory conditions that can contribute to the development of shoulder joint arthrosis.
Symptoms of shoulder joint arthrosis can develop gradually and include:
Pain in the shoulder joint, which may worsen during movement.
Limited shoulder mobility and difficulty lifting the arm.
Creaking or grinding in the joint during movement.
Poor sleep quality due to pain.
Avoid lifting heavy objects or repetitive movements that could worsen the pain. Find alternatives or use aids that make certain tasks easier to perform. A healthy lifestyle that includes a balanced diet, exercise, and maintaining a healthy weight can help reduce symptoms of arthrosis and improve overall health.
Treatment includes pain relief, physiotherapy, lifestyle adjustments and, in severe cases, surgery. Physiotherapy plays a key role in the treatment of shoulder arthrosis, as it helps manage pain, improve joint mobility, and strengthen the muscles of the shoulder girdle.
Shoulder impingement syndrome
Shoulder impingement syndrome is a condition where soft tissues, such as tendons, ligaments, and bursae, become irritated and compressed between bony structures in the shoulder joint.Causes include repetitive movements or activities that involve raising the arm above the head (such as throwing, swimming, or tennis), poor posture and incorrect body mechanics when performing certain movements, muscle imbalances, and weakness of the shoulder girdle muscles.
In shoulder impingement syndrome, soft tissues, such as the rotator cuff tendons (especially the supraspinatus tendon) or the synovial membrane, become compressed between the acromion (the protrusion of the shoulder blade) and the head of the humerus. This irritation leads to inflammation, oedema, and subsequent pain and limited mobility.
Symptoms and clinical signs present as:
Pain that is usually localised on the outside of the shoulder and worsens when raising the arm or performing overhead activities.
Limited mobility: Difficulties raising the arm or extending the arm forward.
Muscle weakness: A feeling of weakness in the shoulder muscles, which can affect everyday activities.
Sensitivity and swelling.
Physiotherapy is a key part of treating shoulder impingement syndrome. Physiotherapists help you reduce pain, recover faster, strengthen the muscles in the shoulder area, and restore function. Anti-inflammatory medications or, in some cases, corticosteroid injections into the shoulder joint may be used to reduce pain and inflammation.
In cases where conservative methods do not provide sufficient relief, the doctor may opt for surgery to release the impinged tissue and correct any structural changes in the shoulder joint.
Clavicle injuries
A clavicle fracture is one of the most common injuries to the musculoskeletal system, often occurring in people of all ages. The clavicle (Latin: clavicula, meaning “little key”) is a key bone, important for proper function of the shoulder joint and upper extremity.
It connects the chest to the shoulder girdle and serves as a support for maintaining the correct position of the shoulder. The clavicle is attached to the sternum medially and to the acromion and coracoid laterally by strong ligaments that are stronger than the bone itself. This connection allows for stability and mobility of the shoulder joint.
Clavicle fractures are classified into three main types, depending on the location of the fracture:
Fractures of the middle third of the clavicle: These are the most common clavicle fractures, in which the fracture occurs in the middle part of the bone. These fractures often occur because of a fall on an outstretched arm or a direct blow to the clavicle.This results in the displacement of the main broken parts of the bones, which may overlap, making it difficult for the fracture to heal properly.
Fractures of the lateral section of the clavicle: In these fractures, damage occurs to the bone at its distal (end) section, which is connected to the acromion. These fractures also occur because of a fall on an outstretched arm or a direct blow to the clavicle. A fracture of lateral section of the clavicle can cause instability of the shoulder joint.
Fractures of the medial section of the clavicle: These are the least common clavicle fractures, where the fracture occurs at the proximal (medial) section of the bone that connects to the sternum. These fractures usually occur because of a strong blow to the clavicle or a fall on the shoulder. Fractures of the medial section of the clavicle can be serious, as they can cause damage to nearby structures, such as blood vessels or lungs.
Did you know that a clavicle fracture is one of the most common bone fractures, especially in sports activities and traffic accidents?
When a clavicle fracture occurs, the two broken sections of the bone move towards each other due to the weight of the upper extremity and the pull of the muscles.During the healing process, the fractured bone may heal in a misaligned position, which can lead to permanent instability of the shoulder joint. This can limit the mobility of the upper extremity and cause pain and disruption in everyday activities.
Treatment for a clavicle fracture depends on the type and severity of the fracture, as well as the patient’s age and activity level. For minor fractures of the middle third of the clavicle, where there is no significant displacement of the broken bone parts, conservative treatment may be used, such as wearing a splint to support and immobilise the shoulder joint, followed by physiotherapy rehabilitation.
In the case of fractures with greater displacement of the broken parts of the bone or in fractures of the lateral and medial section of the clavicle, surgery is often necessary, which may include the use of plates and screws to stabilize the bone – after surgery, physiotherapy treatment is also necessary to restore optimal function to the shoulder.
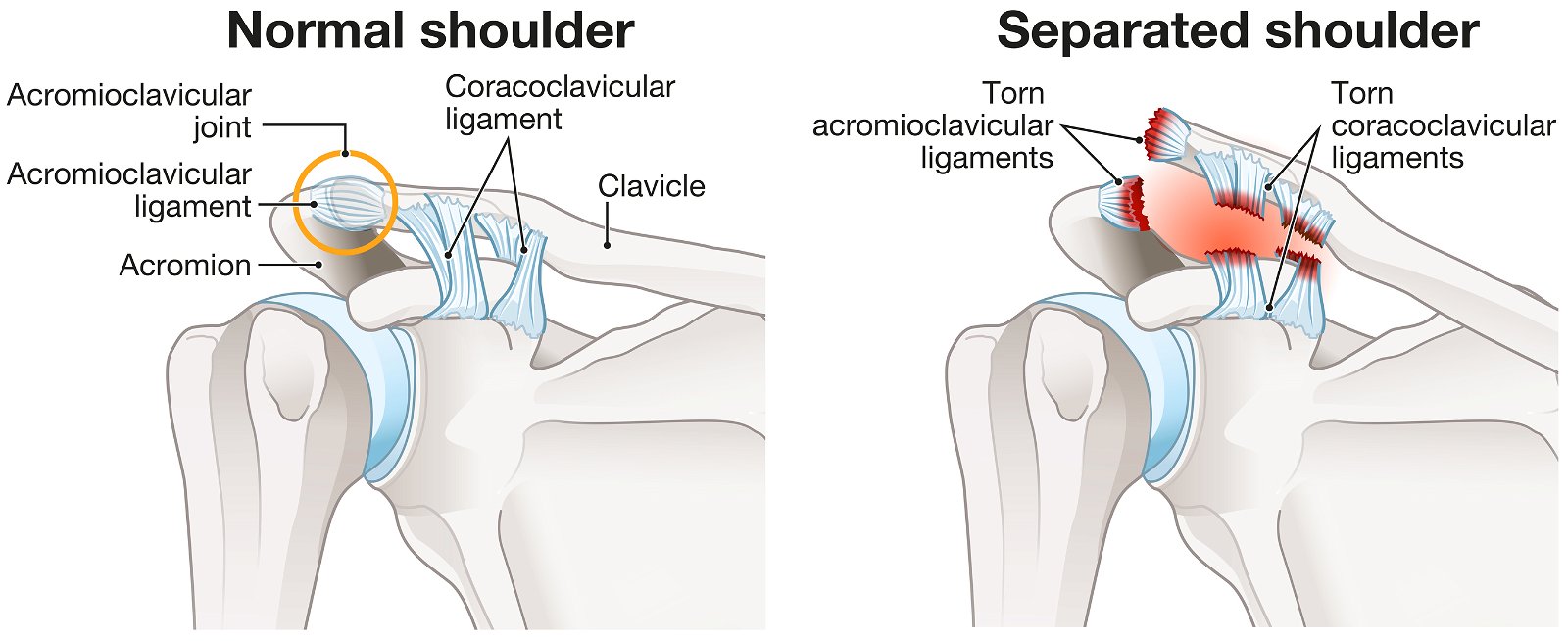
Acromioclavicular syndesmolysis is an injury that occurs in the shoulder joint area and affects the connection between the clavicle and the scapula. This type of injury often affects athletes, especially in contact sports such as football, rugby, basketball, handball, and martial arts. However, acromioclavicular syndesmolysis can also occur with sudden falls on the shoulder or a blow to the shoulder joint.
The main symptom of acromioclavicular syndesmolysis is pain in the shoulder area, which can spread to the neck, arm, and back. The injured area is often swollen and tender to the touch. In some patients, there may be a visible deformity of the joint, with the clavicle protruding upwards.
The diagnosis is usually made based on the history of the injury, physical examination, and imaging studies. An X-ray of the shoulder joint is a common imaging study that allows assessment of the severity of the injury and the degree of displacement of the bones.
Acromioclavicular syndesmolysis is usually classified into grades based on the severity of the injury. There are three main grades:
Grade 1: A mild injury that involves a strain or partial tear of a ligament. The joint is tender and swollen, but there is no observable deformity.
Grade 2: A moderate injury with a full tear of the ligament. The joint is swollen, painful and deformed. The clavicle is elevated and protrudes from the plane of the shoulder joint.
Grade 3: A severe injury with a full tear of the ligament and displacement of the bone. The joint is severely swollen, painful and deformed. The clavicle is significantly elevated above the plane of the shoulder joint.
Treatment for acromioclavicular syndesmolysis depends on the injury grade. For mild injuries (grade 1), conservative treatment is usually recommended, which includes rest, immobilisation of the joint with a splint, reduction of swelling with ice, anti-inflammatory medications, and physiotherapy to restore strength and mobility.
For moderate to severe injuries (grades 2 and 3), surgery is sometimes recommended. Surgery may involve reattaching the bone using screws, plates, or artificial ligaments.
After surgery, there is a period of rehabilitation that includes physiotherapy to restore strength, stability, and mobility of the joint. The goal of physiotherapy rehabilitation is to restore shoulder joint mobility, strengthen muscles, improve joint stability and function, and prevent re-injury.
Axillary nerve injury
The axillary nerve is one of the important major branches of the brachial plexus, which supplies the muscles and skin in the shoulder girdle area. An axillary nerve injury can affect the function and mobility of the shoulder joint and cause pain and loss of muscle strength in this area.
Did you know? The axillary nerve is one of the branches of the brachial plexus, which originates in the spinal cord in the neck (C5–C6) and passes through the armpit (axilla – hence its name) on its way to the shoulder joint. It is responsible for innervating the deltoid muscles (the muscle on the top of the shoulder) and teres minor (the muscle on the back of the shoulder).
An axillary nerve injury can occur due to various causes:
Shoulder injuries: Falls, blows, or sprains of the shoulder can cause compression, stretching, or rupture of the nerve in the shoulder girdle area.
Repetitive use of the shoulder joint: Certain occupational activities or sports that require repetitive lifting of heavy loads or frequent rotation of the shoulder can cause wear and tear or inflammation of the axillary nerve.
Shoulder joint dislocation: A shoulder dislocation can lead to compression or injury to the axillary nerve in the area of the joint.
Symptoms of axillary nerve injury can vary depending on the severity of the injury. Some of the common symptoms include:
Pain: Patients often report pain in the shoulder joint area, which may radiate towards the upper arm.
Limited mobility: Nerve damage can cause impaired mobility and difficulty lifting or laterally raising the arm.
Muscle weakness: Axillary nerve damage can cause weakness of the shoulder girdle muscles, which manifests as difficulties when lifting and holding the arm in a horizontal position.
Numbness or tingling: Some patients may experience numbness or tingling in the shoulder girdle or upper arm.
Treatment for axillary nerve injury depends on the severity of the injury and the patient’s individual needs. Physiotherapy plays a key role in rehabilitation after axillary nerve injury. The goal of physiotherapy is to improve muscle strength, mobility and coordination, and reduce pain. Surgical approaches have proven unsuccessful in most cases.
WHEN TO OPT FOR MEDICOFIT DIAGNOSTIC THERAPY?
When shoulder pain or potential swelling persist for several days, it is necessary to undergo diagnostic therapy.
When you have a feeling that your shoulder is unstable or has significantly reduced mobility, especially after an injury.
If you have previously had problems with your shoulder joint and the symptoms are recurring, this means that the injury was not properly treated or that a new injury has occurred.
At MEDICOFIT clinic, we provide patients with shoulder pain with scientifically supported specialist physiotherapy, which begins with booking a diagnostic therapy appointment.
Comprehensive shoulder pain treatment at MEDICOFIT clinic
Physiotherapy rehabilitation of the shoulder joint begins with diagnostic therapy, which is the basis for the subsequent individualised physiotherapy and kinesiology treatment programme.
The length of physiotherapy rehabilitation varies depending on the individual’s level of physical fitness, diagnosis, cause of the disease, and intensity of symptoms.
Diagnostic therapy
A physiotherapist specialising in the treatment of the shoulder joint conducts a thorough examination, obtaining information about the history of the disease, the duration of symptoms, and any other pathologies present.
A physical examination is performed during the examination to obtain the following information:
inspection and palpation of the skin and soft tissue structures (colour, temperature, skin perspiration, muscle stiffness),
range of motion in the shoulder joint (the diagnostician will check your active and passive range of motion in all directions and confirm the presence of a capsular pattern),
muscle function (through muscle testing we determine strength, endurance, atrophy and potential muscle imbalances),
pain assessment (whether it is spot pain, radiates, how long is it present, is it sharp, dull or burning pain in the shoulder, VAS scale),
inflammation and swelling (swelling is observed, possible deformation of anatomical structures),
irregular movement patterns (cause improper distribution of forces in the body and increased strain on structures; often appearing because of pain),
neurological condition of the body (motor function, sensory function and reflex changes),
specific tests (determine the location of the injury or the source of the pain).
Diagnostics additionally includes an examination of the cervical spine, shoulder blade, elbow joint, wrist, and fingers.
For certain individuals, referral for diagnostic imaging (X-ray, ultrasound, magnetic resonance imaging) is necessary.
Acute physiotherapy
Physiotherapy treatment includes the use of manual therapy, instrumental devices, and special therapeutic training.
It primarily focuses on symptom control (reducing pain, swelling and inflammation) and faster tissue healing using state-of-the-art instrumental devices:
Diamagnetic therapy
TECAR therapy
Laser therapy
HiTop high-tone electrotherapy
Manual therapy (joint mobilisation, trigger point therapy, myofascial release) is used to release muscle tension, restore proper joint sliding, and restore function to the affected area.
With special therapeutic training and active mobility training we achieve full range of motion in the shoulder joint and open up the subacromial space.
Once full mobility is achieved, strength training begins to correct muscle imbalances and to ensure additional stabilisation of the shoulder joint. The purpose of the training is to relax shortened muscles and strengthen weak ones.
The goals of physiotherapy are to achieve sufficient range of motion, adequate muscle strength, joint stability, and coordination of movement.
WHY CHOOSE SPECIALIST PHYSIOTHERAPY TREATMENT?
We ensure high treatment success and long-term results.
Proven reduced need for surgery!
We offer state-of-the-art non-invasive treatment methods that provide optimal conditions for the healing of shoulder joint injuries.
Comprehensive treatment of shoulder pain at MEDICOFIT clinic is recommended by numerous renowned orthopaedic surgery specialists.
Post-acute kinesiology
Once the physiotherapy treatment goals are achieved, the kinesiology phase begins, which leads the individual to the physical fitness level they had before the injury.
Progressive physical training eliminates compensatory movements that have arisen as a result of pain or lifestyle, and establishes correct functional patterns that enable optimal movement function of the body (properly distributed forces and loading of structures).
Correct movement of the scapula, scapulothoracic joint, and appropriate postural control are established, enabling correct functional movement.
The main goal of the kinesiology phase of treatment is to fully restore shoulder function.
Preventive kinesiotherapy
After treatment is complete, it is crucial that shoulder pain does not recur.
At MEDICOFIT clinic we have implemented a preventive kinesiology programme that successfully prevents the recurrence of old injuries and the occurrence of new injuries.
Targeted strength training keeps the body functioning optimally and prepares it for everyday loads.
DANGERS AND PITFALLS OF DELAYED REHABILITATION
MEDICOFIT specialists
Untreated shoulder pain can cause decreased shoulder mobility and function, leading to stiffness and a reduced ability to perform normal movements.
If pain causes limited mobility, muscle atrophy may occur, which means loss of muscle mass and strength.This can further weaken the shoulder and make recovery more difficult.
If shoulder pain is not treated in a timely manner, the condition can worsen to the point where surgery is required.
Inadequate or delayed rehabilitation seriously jeopardises an individual’s long-term physical health and is the main culprit for unsuccessful results and permanent movement limitations.
Exercises for shoulder pain
Below, we also present some effective exercises that you can incorporate into your routine to reduce discomfort and regain flexibility and strength in your shoulder joint. Performing these exercises correctly will help you improve your quality of life and prevent further injuries.
Important notice
• The exercise can be performed in numerous modifications and different load regimens; proper execution will be prescribed by a MEDICOFIT physiotherapy specialist for shoulder pain rehabilitation as part of your comprehensive treatment. • If you have shoulder joint problems, please book an diagnostic therapy appointment before performing the exercise. The exercise may also be contraindicated. • Always do the exercise strictly according to the prescribed regimen and as demonstrated by the physiotherapy specialist for shoulder joint rehabilitation and disorders. • We recommend the exercise as part of guided, comprehensive specialist physiotherapy for shoulder rehabilitation. • If you perform the exercise independently without the supervision of a physiotherapy specialist, we are not responsible for potential symptomatic responses.
Exercise no. 1: One-arm internal rotations with elastic band + arm push up
Exercise no. 2: Isometric one-arm external rotation with elastic band + walking sideways
Exercise no. 3: Alternating one-arm flexion and abduction of the shoulder while lying down + elastic band
Frequently asked questions about shoulder pain
When is it necessary to see a doctor for shoulder pain?
A visit to the doctor is recommended when:
the shoulder pain is unbearable,
the injury causes a severe visible deformity,
the pain is accompanied by fever, fainting, nausea,
there is increased swelling or bruising in the shoulder,
referred shoulder pain accompanied by chest pain may be a sign of heart problems that require immediate medical attention!
Is it recommended to do exercises despite shoulder pain?
Yes, it is recommended to actively perform exercises despite shoulder pain. It is crucial to select the correct exercises and to do the exercises properly, so a visit to a physiotherapist is recommended!
How can I prevent chronic shoulder pain?
Timely determination of the cause of pain (through a diagnostic examination) and appropriate physiotherapy treatment prevent worsening of shoulder pain!
Book an appointment for shoulder joint rehabilitation
Abrams R, Akbarnia H. Shoulder Dislocations Overview. [Updated 2022 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459125/
Brockmeyer, M., Tompkins, M., Kohn, D. M., & Lorbach, O. (2016). SLAP lesions: a treatment algorithm. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA, 24(2), 447–455. https://doi.org/10.1007/s00167-015-3966-0
org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. Shoulder pain: Overview. 2020 Feb 13. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554693/
May, T., & Garmel, G. M. (2022). Rotator Cuff Injury. In StatPearls. StatPearls Publishing.
St Angelo JM, Fabiano SE. Adhesive Capsulitis. [Updated 2022 Nov 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532955/
This website uses cookies so that we can provide you with the best user experience possible. Cookie information is stored in your browser and performs functions such as recognising you when you return to our website and helping our team to understand which sections of the website you find most interesting and useful.
Strictly Necessary Cookies
Strictly Necessary Cookie should be enabled at all times so that we can save your preferences for cookie settings.
3rd Party Cookies
This website uses Google Analytics to collect anonymous information such as the number of visitors to the site, and the most popular pages. Keeping this cookie enabled helps us to improve our website.
Please enable Strictly Necessary Cookies first so that we can save your preferences!
Additional Cookies
This website uses the following additional cookies:
(List the cookies that you are using on the website here.)
Please enable Strictly Necessary Cookies first so that we can save your preferences!