The most common of the spinal disorders is a hernia of the intervertebral disc. There are several types of hernias in the spine (disc hernia, disc protrusion, disc extrusion, disc sequestration, rupture hernia) and one of them is Schmorl’s nodes or intravertebral hernia.
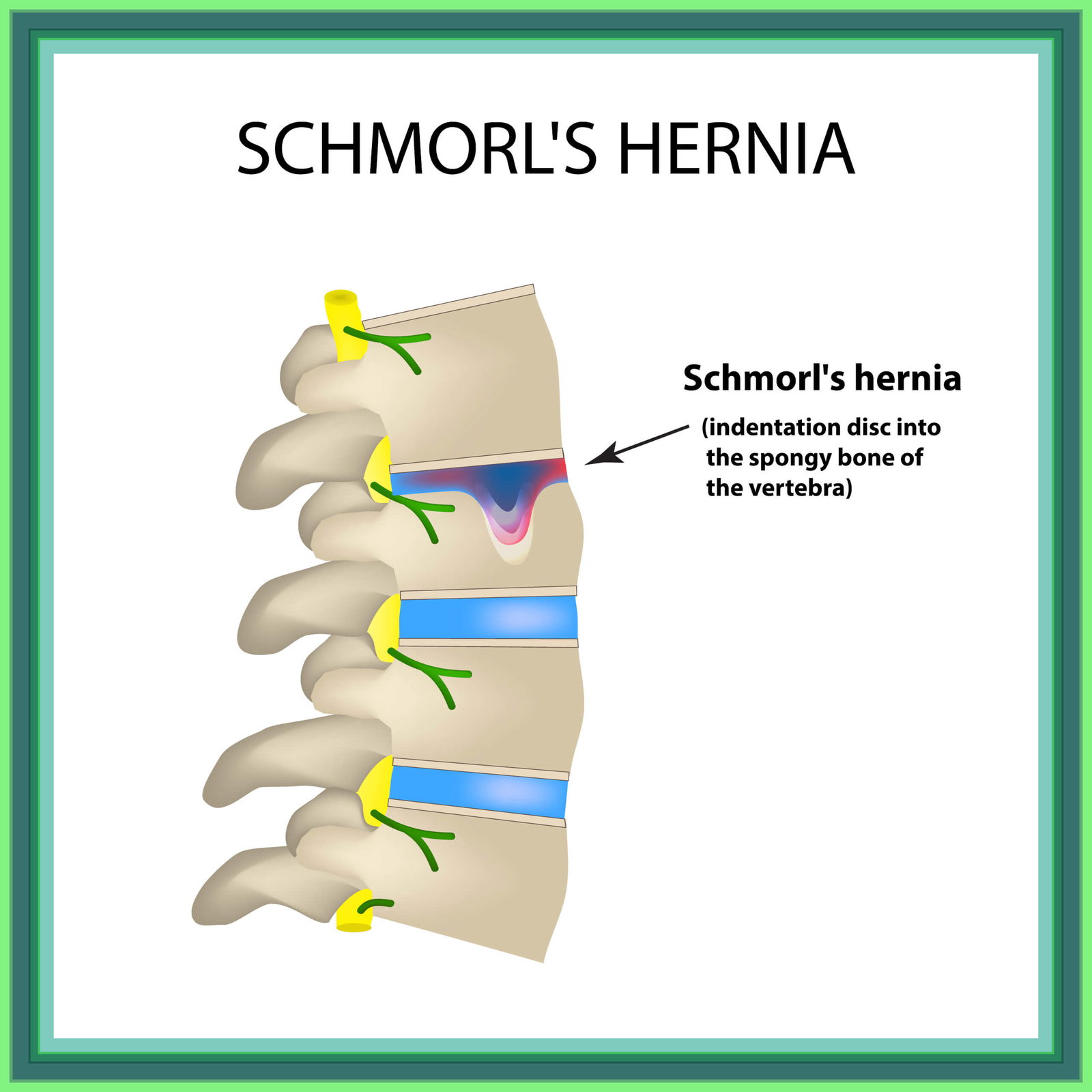
Schmorl’s nodes is caused by an intervertebral disc bulging upwards or downwards into the vertebral body. It is a common condition affecting up to 75% of the population, from adolescents to the elderly. The average age of an individual with Schmorl’s nodes is 55 years.
The cause of the disease is currently unknown, but the problem is caused by a weakened intervertebral disc, degeneration of the vertebra or an autoimmune reaction.
The main difference between Schmorl’s nodes and a disc hernia is in the direction of the bulging disc, i.e. the disc hernia bulges sideways and occludes the nerve root, which causes neurological symptoms – burning pain and a tingling and numb sensation radiating to the upper/lower limb.
Schmorl’s nodes is dangerous because it is asymptomatic, meaning that its symptoms are not felt until it is too late and chronic pain and problems develop. When symptoms are felt, individuals report sharp pain in the spine.
Spinal pain and mobility problems are the most common symptoms for a visit to a physiotherapist to diagnose the cause of your problems and to set up further physiotherapy treatment.
The spine is made up of 33 vertebrae, divided into cervical, thoracic, lumbar and sacral regions. The vertebrae are intergrown in the sacral (pelvic) region. The vertebrae are anatomically built to provide support and mobility to the whole body and to protect the spinal canal (spinal cord).
From the cervical to the first sacral vertebrae, the vertebrae are separated from each other by intervertebral discs (discs). The intervertebral disc has a soft nucleus (nucleus pulposus) and the armour around the soft nucleus is fibrous (tissue made of collagen). The primary function of the intervertebral disc is to transmit the forces and loads that are exerted on the spine on a daily basis.
The spinal cord runs from the skull down through the vertebrae of the spine and carries messages between the body and the brain via its nerves. Often, nerve structures are affected when there is a bulging of the intervertebral disc, causing thinning of the spinal canal (spinal stenosis) or compression of the nerve roots (sciatica).
What happens over time when the spine is subjected to overload tensile forces that it is anatomically unable to withstand?

The mechanism of Schmorl’s nodes is currently unknown. The most likely cause is stress loads imposed on a too weak intervertebral disc. The intervertebral disc becomes affected for reasons such as degenerative structural spinal changes, infection, metabolic disease, tumour formation or osteoporosis.
Scientific studies have shown a correlation between the occurrence of a Schmorl’s nodes and the degree of degeneration of the intervertebral disc.
Schmorl’s nodes occurs when excessive loads are applied to the spine and the soft core of the intervertebral disc bulges upwards or downwards into the bony vertebrae of the spine. The intervertebral disc changes shape and becomes less susceptible to the stresses placed on the spine.
Common causes of Schmorl’s nodes are tensile vertical loads such as walking, prolonged standing, stooping from a height and old age. Adolescents who develop juvenile kyphosis are more susceptible to developing Schmorl’s nodes later on.
Schmorl’s nodes is caused by an acute traumatic injury to the spine and is distinguished from the chronic form on the basis of MRI imaging, as there is no inflammation present in an acute hernia.
Schmorl’s nodes occurs more frequently in the lumbar region than in the cervical or thoracic regions of the spine.
In most cases, Schmorl’s nodes is asymptomatic, meaning that the individual does not experience any symptoms.
The symptoms of chronic pain are caused by inflammation that develops in the vertebra. Inflammation occurs when the soft core bulges and presses against the bone marrow of the vertebra.
Acute pain and symptoms (soreness, limited mobility, reduced muscle strength) quickly develop into chronic pain that limits daily functioning.
Schmorl’s nodes rarely presses on a nerve root causing a burning radiating pain in the lower/upper limb.
What to do when you feel the first signs of spinal pain? A specialist examination by a diagnostic physiotherapist is recommended.
A specialist diagnostic examination for acute and chronic lower back pain is essential to determine the correct physiotherapy treatment.
The diagnostic examination is carried out by a physiotherapist diagnostician and includes:
- Anamnesis,
- A detailed medical history,
- Assessment of arthrokinematics,
- Assessment of muscle capacity and imbalances,
- Pain assessment,
- Spinal load capacity,
- Functional body movement patterns,
- Biomechanics of gait,
- Specific tests.
Disrupted functional movement patterns have a negative impact on all body structures, which weaken over time and become more susceptible to injury and pain.
Particular attention shall be paid to measuring the load capacity of the spine in all postures to reveal abnormalities in the way it is loaded.
Primary causes such as wear and tear of the facet joints, arthrosis of the spine, degenerative changes of the intervertebral disc lead to the formation of a Schmorl’s nodes.
Comprehensive diagnostics focuses on the discovery of the cause of a Schmorl’s nodes and the subsequent targeted treatment of the hernia. This is the only real way to eliminate your pain.

The diagnosis of Schmorl’s nodes is confirmed by diagnostic imaging – magnetic resonance imaging (MRI) by a medical specialist (neurosurgeon or orthopaedic surgeon).
Based on the information obtained about your body, an individually tailored physiotherapy programme is set up to address the personal cause of your problems and the resulting limitations.
Physiotherapy and kinesiotherapy treatment
The physiotherapy programme for the treatment of Schmorl’s nodes includes manual therapy, joint mobilization, specialized exercise and the use of instrumentation. It consists of several stages, which are tailored according to your acute or chronic pain, the limitations of the disease and your body, and your abilities.
Acute or chronic spinal pain resulting from Schmorl’s nodes is treated holistically. The holistic physiotherapy treatment is aimed at eliminating the symptoms and the cause of the disease. By eliminating the cause, the risk of future recurrence of symptoms is reduced.
Actively targeted physiotherapy rehabilitation successfully restores the original motor function of the body and its posture, improves muscle strength and muscle proportion, increases flexibility and mobility, and maintains the correct gait pattern.
The latest assistive technology has proven to be extremely effective in treating the symptoms of hernias. LASER therapy, ultrasound therapy, TECAR therapy and HiTOP electrotherapy work by causing the body to heal itself more quickly, significantly reducing pain, inflammation and the resulting swelling.

Physiotherapy rehabilitation focuses on progressive stabilization exercises (in the directions of antiflexion, anti-extension, anti-rotation and anti-lateroflexion) which improve the mobility and strength of the body’s core from which all correct movement originates.
The programme involves the correct establishment of functional movement patterns, which are encouraged through intensive mobility exercises. The daily stresses placed on the spine in all movements (picking up from the floor, sitting for long periods, carrying heavy loads, etc.) make it important to strengthen muscular strength and endurance.
It is important to analyse in detail how you perform your daily movements and to learn how to correctly perform and adapt movements that cause pain and additional damage.
Kinesiology phase
The kinesiology programme for Schmorl’s nodes starts after the acute physiotherapy phase of treatment and guides the individual to successfully complete specific rehabilitation tests. It includes specialized training (neuromuscular training, balance and proprioceptive training, muscular strength and endurance training) that maintains muscular strength, flexibility and general body condition. It focuses on the preventive maintenance of the motor function of the body and the prevention of new injuries.
Specific tests are repeated before the end of the treatment to give us an insight into the progress of the rehabilitation.
Book your physiotheraphy appointment now!
Can I prevent Schmorl’s nodes?
Maintaining the correct load capacity and muscle strength in the spine, avoiding incorrect daily movements and being at the right weight will reduce the chance of developing a Schmorl’s nodes.
Effective physiotherapy treatment prevents the progression of a pre-existing Schmorl’s nodes.
Schmorl’s nodes is a special type of hernia that causes the least problems because it is asymptomatic. When acute symptoms in the form of sharp pain occur, they are caused by a direct traumatic blow to the spine. Chronic symptoms, on the other hand, are caused by a long-standing weakened intervertebral disc bulging upwards or downwards into the adjacent vertebra.
Schmorl’s nodes is confirmed by a diagnostic examination and diagnostic imaging (MRI), which identifies whether the condition is of acute or chronic origin. A chronic Schmorl’s nodes causes inflammation in the vertebra, whereas an acute condition does not.
It is a common condition, affecting 38-75% of the world’s population, according to recent data. According to some data, men are more susceptible to developing Schmorl’s nodes than women.

Schmorl’s nodes is in most cases treated conservatively (physiotherapy and medical treatment/medication), as surgery is rarely indicated/necessary.
The integrated medical treatment includes a correct diagnosis through a diagnostic examination, individualised physiotherapy treatment and kinesiotherapy.
Physiotherapy treatment of Schmorl’s nodes is completed when the degenerative processes in the body have been positively reduced, the weakness of the spinal muscles and stabilisers of the trunk have been eliminated, the mobility in the body has been increased, and the correct posture has been established, resulting in the correct loading of the structures in the spine.
- Sadiq, I.M. Lumbar spine Schmorl’s nodes; prevalence in adults with back pain, and their relation to vertebral endplate degeneration. Egypt J Radiol Nucl Med50, 65 (2019). https://doi.org/10.1186/s43055-019-0069-9
- Kim HS, Raorane HD, Sharma SB, Wu PH, Jang IT. Infected Schmorl’s node: a case report. BMC Musculoskelet Disord. 2020 May 2;21(1):280. doi: 10.1186/s12891-020-03276-4. PMID: 32359347; PMCID: PMC7196219.
- Abu-Ghanem S, Ohana N, Abu-Ghanem Y, Kittani M, Shelef I. Acute schmorl node in dorsal spine: an unusual cause of a sudden onset of severe back pain in a young female. Asian Spine J. 2013 Jun;7(2):131-5. doi: 10.4184/asj.2013.7.2.131. Epub 2013 May 22. PMID: 23741552; PMCID: PMC3669699.
- Ekşi, M.Ş. et al. (2022) Schmorl’s nodes could be associated with intervertebral disc degeneration at upper lumbar levels and end-plate disease at lower lumbar level in patients with low back pain, Journal of Clinical Neuroscience. Elsevier. Available at: https://www.jocn-journal.com/article/S0967-5868(22)00160-6/fulltext
- Williams, F.M.K., Manek, N.J., Sambrook, P.N., Spector, T.D. and Macgregor, A.J. (2007), Schmorl’s nodes: Common, highly heritable, and related to lumbar disc disease. Arthritis & Rheumatism, 57: 855-860. https://doi.org/10.1002/art.22789
- Sonne-Holm S, Jacobsen S, Rovsing H, Monrad H. The epidemiology of Schmorl’s nodes and their correlation to radiographic degeneration in 4,151 subjects. Eur Spine J. 2013 Aug;22(8):1907-12. doi: 10.1007/s00586-013-2735-3. Epub 2013 Mar 16. PMID: 23503898; PMCID: PMC3731494.








