Did you know that meniscus injury is the leading reason for arthroscopic knee joint surgery? For example, in the USA, 400,000 meniscus surgeries are performed every year. You probably did not know that meniscus injuries can be asymptomatic, i.e. painless, but still dangerous if not treated properly.
The first choice of treatment for all types of meniscus injuries is specialised physiotherapy and is a priority over surgical treatment for approximately 80% of all meniscus injuries.
At MEDICOFIT clinic, we are aware that the patient’s understanding of their condition is the key to successful rehabilitation, as only then will the patient – bombarded with all sorts of information and expert opinions – be able to make the right decision regarding the type of treatment.
Rehabilitation of meniscus injuries is complex and requires careful planning and execution. Prolonged immobility and rest are contraindicated, as they contribute to the development of movement limitations. Early rehabilitation is needed, which includes maintaining mobility and strength of the knee joint.
How does a meniscus injury occur?
The meniscus is most often injured in athletes, such as football, basketball, handball players, as well as in martial artist and skiers. It is often injured by a fall on the knee or a blow to the knee. It is typical for meniscus injuries to have two mechanisms of origin.
The meniscus can be damaged gradually due to long-term overuse, in which case it is a degenerative origin of meniscus damage. The meniscus can also be injured by trauma, in which case it can be a contact or non-contact injury. The mechanism of meniscus injury is usually forceful rotation of the knee while the foot is fixed.
A traumatic meniscus injury is characterised by severe pain, but it does not necessarily result in a rupture or tear. However, it is common for traumatic injury to the meniscus to cause inability to bear weight on the leg and swelling of the knee.
The individual can often hear a pop and feel that something has “torn off”, in which case it is probably a more extensive injury, e.g. a meniscus rupture. It is also typical for sports-related meniscus injuries that athletes with a higher pain threshold can continue their sports activity.
Degenerative meniscus injury occurs because the meniscus loses its resistance due to wear and gradually becomes thinner, which then results in minor tears or cracks. In degenerative meniscus injuries, a free fragment of the meniscus (loose body) can often form, which detaches from the main structure and “floats” independently in the joint. Below we will also explain meniscus catching.
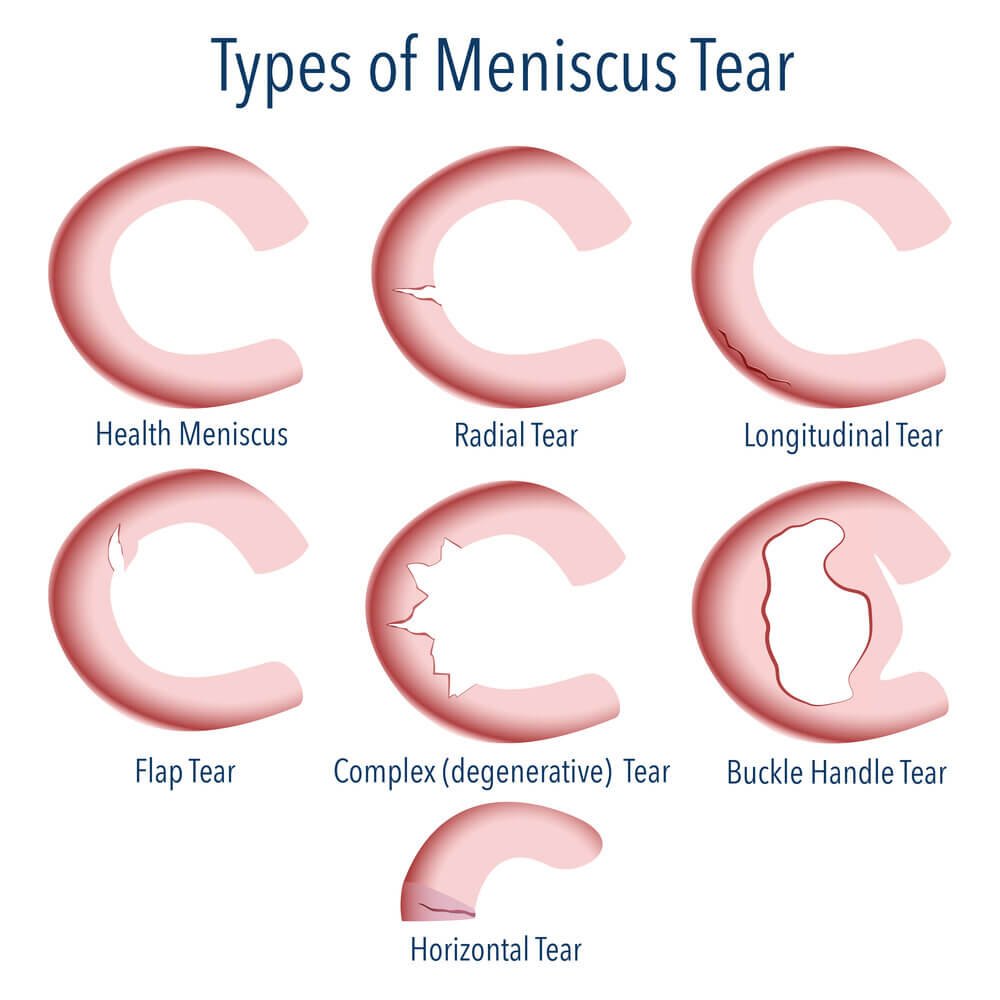
Because of its complex structure, the meniscus can be damaged in many different ways. It can, for example, be simply compressed, it can be torn at the periphery in the red zone (the zone where there is blood supply and the meniscus can heal), it can be torn in half, there can be a loose part of the meniscus, the edge of the meniscus can simply be “rolled back“, a characteristic injury of the medial meniscus is a bucket handle tear, when the meniscus splits into two parts because a longer longitudinal tear, and an empty space in the shape of the letter C is created in between. We know at least six different basic injuries of the meniscus and subsequently at least 12 well-known sub-variations.
WHY CHOOSE SPECIALIST PHYSIOTHERAPY TREATMENT?
We ensure high treatment success and long-term results.
Up to 85% lower risk of surgical treatment of a meniscus injury!
We offer state-of-the-art non-invasive treatment methods that provide optimal conditions for the healing of injuries.
Comprehensive treatment of meniscus injury at MEDICOFIT clinic is recommended by numerous renowned orthopaedic surgery specialists.
Which meniscus is more often injured: medial or lateral?
The medial meniscus is injured up to six times more often than the lateral meniscus. The difference occurs primarily because of the specific anatomical structure of the attachments, which is described at the beginning of the article. The medial meniscus is more strongly attached to the knee joint, has three points of attachment, and a lower degree of mobility than the lateral meniscus.
The medial meniscus grows on the MCL (medial collateral ligament), which is a commonly injured knee ligament in athletes. The lateral meniscus is more mobile than the medial meniscus, so it is injured less frequently, but injuries to the lateral meniscus are typically more complex and more often treated surgically. The lateral meniscus is often damaged when there is a severe traumatic injury to the anterior cruciate ligament.
How does the meniscus even function?
The meniscus primarily provides structural integrity to the knee joint, and it can also be called a body’s “shock absorber” or a cushion. The meniscus bears more than 50% of the total load of the knee and is an important “bodyguard” of the cartilage surfaces. When meniscus fails, the way is open to cartilage surface damage. Accelerated wear of cartilage surfaces of the knee often occurs after meniscus injuries in combination with inadequate muscle statics or inadequately performed rehabilitation.
The medial and lateral meniscus provide the knee joint with greater compression resistance through the mechanism of distributing intra-articular load over a larger “gross” surface area. The meniscus aligns the ends of the femur and tibia so that force is transmitted over a larger surface area. It is important to understand that the meniscus primarily provides structural integrity for vertical loads, while greater rotational, valgus, and varus loads are the “Achilles heel” of the meniscus.
The meniscus is also an important “lubricant” for the knee joint. Synovial fluid is the main lubricant for joints, and the meniscus distributes synovial fluid in the knee in proportion to the areas of load.
Did you know that the meniscus is also a knee stabiliser? The meniscus is indirectly an important stabiliser of the knee joint, as it enables more stable function of the knee joint during movement by distributing vertical loads over a larger gross surface area.
How is the meniscus composed?
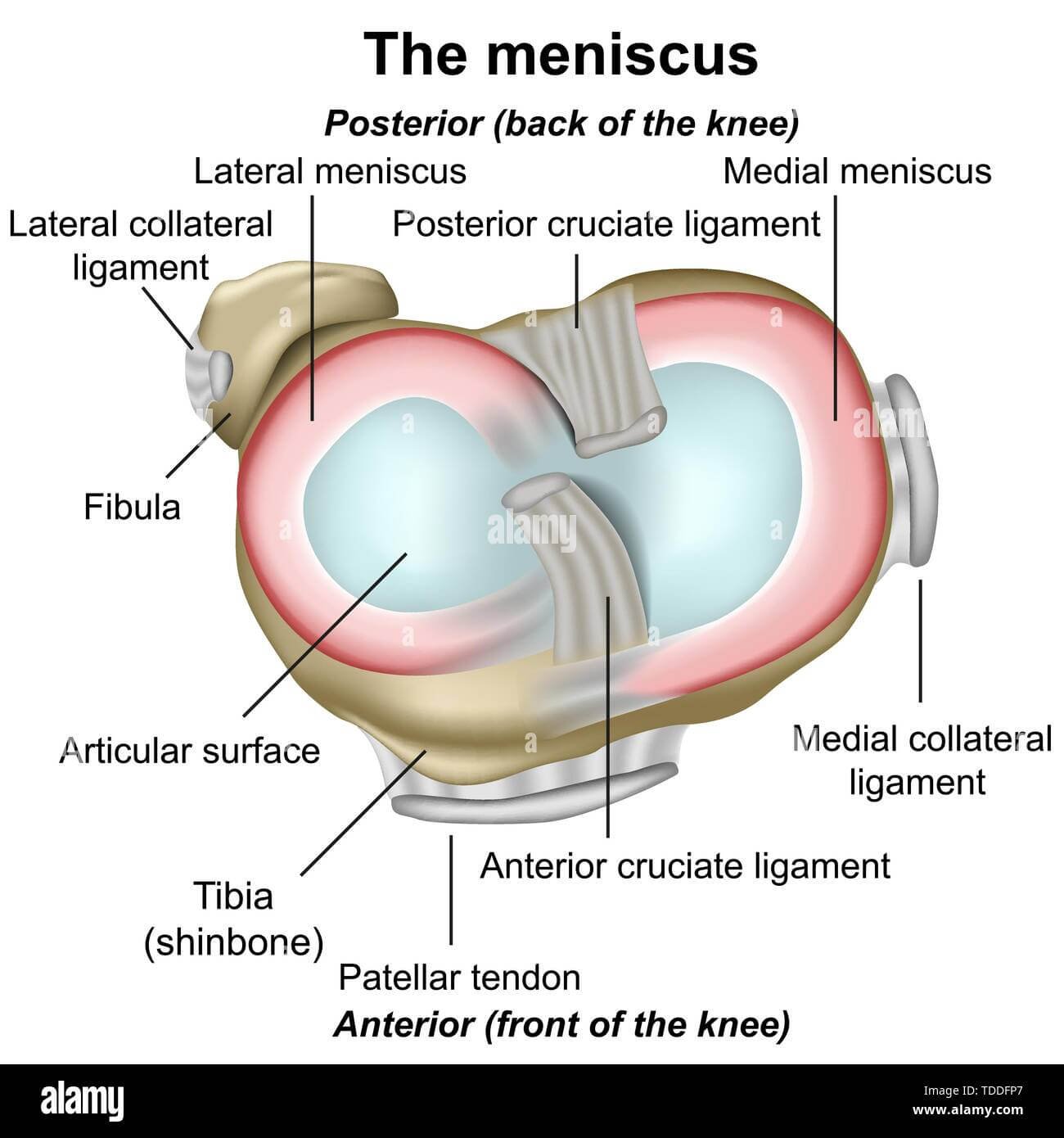
When reading magnetic resonance imaging (MRI) scans, we often encounter interesting terminology related to the meniscus. Below we present the anatomy of the meniscus along with an explanation. The meniscus has a complex anatomy of attachments, which are often the cause of various types of meniscus injuries. When reading medical reports, you will often come across the term “lesion“, meaning injury, and the term “fissure“, meaning crack, and, in relation to meniscuses, also horn, meaning just part of the meniscus. The anterior horn refers to the front part of the meniscus. The posterior horn refers to the back part of the meniscus.
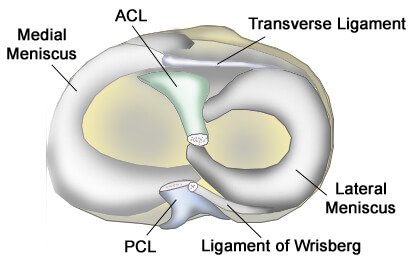
The medial and lateral meniscus are connected inside the knee by the transverse ligament.
The semimembranosus muscle (hamstring muscle) and the quadriceps femoris muscle (the anterior thigh muscle) both attach to both menisci.
Medial meniscus
The medial meniscus is approximately 4.4 centimetres long, 3.5 centimetres wide, and covers 50–60% of the surface of the medial plateau of the tibia, and the anterior horn of the meniscus (the front part) attaches to the anterior region of the tibia.
The medial meniscus is thickest at the posterior horn (back part) and becomes thinner towards the anterior horn. The posterior horn of the meniscus is most stressed during deep knee flexion. During maximum knee flexion, for example, we notice that the posterior horn of the meniscus can slide over the edge of the tibial plateau, where a large load occurs; therefore, in the acute postoperative phase of meniscus surgery, deep knee flexion is prohibited.
The medial meniscus has a total of three attachments, while the lateral meniscus has only two attachments. The medial meniscus attaches to the anterior aspect of the tibia, the joint capsule, and the medial collateral ligament (MCL), and is generally less mobile and more fixed than the lateral meniscus.
Did you know that the attachment of the medial meniscus has at least five different anatomical variations of the anterior horn and at least four anatomical variations of the posterior horn? This means that our meniscuses are genetically very different, which we at MEDICOFIT clinic are aware of – that is why we tailor the treatment of each meniscus specifically to the individual.
Lateral meniscus
The lateral meniscus is approximately 3.6 centimetres long and 2.9 centimetres wide, but covers a much larger area of the tibial plateau than the medial meniscus – up to 68%. The lateral meniscus is more mobile than the medial meniscus and is injured less frequently. It has only two attachments, which allows it greater mobility.
The anterior (front) attachments of the lateral meniscus are closer together than those of the medial meniscus, and on the front side, the lateral meniscus attaches to the anterior cruciate ligament (ACL). The bone attachments of the anterior and posterior horns of the meniscus are connected with ligaments to the popliteus muscle, which provides lateral stability of the lateral meniscus. In the posterior horn, the back part, the lateral meniscus extends to the posterior cruciate ligament (PCL) via the ligament of Wrisberg.
The lateral meniscus is less firmly attached to the lateral part of the knee than the medial meniscus is to the medial part of the knee, which is the cause of a higher number of medial meniscus injuries. The lateral meniscus can move up to 11 mm during movement.
Did you know that the lateral meniscus also has numerous anatomical variations of attachments, and that in some cases the bone attachment of the posterior (back) horn of the meniscus is completely absent and all posterior stability is provided only by the ligament of Wrisberg?
What symptoms does a meniscus injury cause?
A meniscus tear does not always cause symptoms or problems. In some cases, severe pain and a popping sensation in the knee may occur immediately after the injury. In others, swelling in the knee joint may only develop after a few hours.
The key symptom of a meniscus injury is knee pain, which occurs immediately after the injury. There may be a feeling of catching in the knee and swelling of the joint (inflammation occurs when there is an injury).
There may also be a feeling of weakness in the leg and a feeling that the knee is “giving way”.This occurs due to dislocated or torn meniscus tissue and swelling in the knee, which affects the thigh muscles that support the function of the knee.
Pain is usually felt over the site of the meniscus injury when putting weight on the affected knee and/or when turning the knee, for example when getting in and out of a car. Walking up stairs can be especially painful and can cause increased swelling in the knee.
WHEN TO OPT FOR MEDICOFIT DIAGNOSTIC THERAPY?
When knee pain and swelling after an injury last longer than seven days, it is necessary to undergo diagnostic therapy.
If you notice that you cannot fully extend or bend your knee, or if mobility is limited by pain.
If you have previously had problems with the meniscus and the symptoms are recurring, it means that the injury was not properly treated or that a new injury has occurred.
At MEDICOFIT clinic, we provide patients with scientifically supported specialist physiotherapy for meniscus injuries, which begins with booking a diagnostic therapy appointment.
Meniscus surgery can be performed in the form of a partial meniscectomy, i.e. partial removal of the damaged part of the meniscus, or in the form of meniscus suturing if there is a major injury or tear, often in the case of a bucket handle tear type of meniscus injury. Rehabilitation after meniscus suturing is more complex and has a longer acute phase with a longer period of prohibited load-bearing on the knee.
Mandatory meniscus surgery indications are rare; when mechanical symptoms in the form of knee catching and painful knee skipping are present, surgical treatment is indicated. When the tear is more extensive, surgical treatment in the form of suturing is indicated. Pain alone is not an indication for surgical treatment of the meniscus, just as minor injury or degenerative damage to the meniscus is not a mandatory surgery indication.
Studies between 2012 and 2020 have found that meniscectomy (partial removal of the meniscus) compared to conservative treatment in the form of physiotherapy and kinesiology does not show significant differences in joint function three to five years after the onset of injury or symptoms. Conservative treatment of the meniscus often has better long-term effects for the patient, as it improves their function and reduces the likelihood of progression of meniscus damage.
Meniscus removal means that we are at risk of knee arthrosis and accelerated cartilage wear at the site of removal. In any case, for minor meniscus injuries, the first method of treatment is always physiotherapyand kinesiology.
Surgical treatment of minor lesions and injuries of the meniscus is only recommended when at least a three-month structured treatment in the form of physiotherapy and kinesiology has not significantly improved pain symptoms or swelling of the knee.
Comprehensive treatment of meniscus injuries at MEDICOFIT clinic
At MEDICOFIT clinic, we believe in comprehensive individualised rehabilitation of meniscus injuries, which is why we prepare an individualised treatment programme for each patient.
Treatment in our clinic is done in four phases that are closely related: diagnostic examination, acute physiotherapy, post-acute kinesiology and preventive kinesiotherapy.
Diagnostic therapy
At MEDICOFIT clinic, we perform complete diagnostics of a damaged meniscus and first identify the symptoms and mechanical properties of your meniscus. Physiotherapy and kinesiology treatment methods depend greatly on the type of injury you have.
The examination begins with a thorough interview, where the patient shares information about the history of the disease, the time of onset of knee pain, its duration, factors that influence exacerbation of pain, and other important data that help understand their current condition.
This is followed by a thorough physical examination, which includes inspection and palpation of the knee. During the examination, any swelling, inflammation, tenderness, skin colour, and tissue temperature are assessed.
Mobility and muscle strength measurements: Measurements of joint mobility and arthrokinematics are performed, as well as an assessment of muscle strength. This helps us understand muscle strength, endurance, and muscle function.
Biomechanics of walking and load capacity: An assessment of the knee’s load-bearing capacity and walking biomechanics is performed, which can reveal any deviations from normal patterns.
Functional tests: We can assess the condition of your meniscus with a specific test – the McMurray test (to check for possible meniscus damage).
In some cases, diagnostic imaging, such as magnetic resonance imaging, may be recommended to show the exact location and type of meniscus injury. This is important to determine the extent of injury and rule out possible other diagnoses.
Based on the collected data, the physiotherapist designs an individualised therapeutic programme aimed at managing symptoms and rehabilitating the knee.
Acute physiotherapy
In the event of a meniscus injury, we recommend acute physiotherapy, which should begin no later than seven days after the meniscus injury, ideally three days after the injury. A common mistake patients make is to simply rest and avoid instrumental therapy to promote healing and therapy to maintain muscle activation.
We prioritise active physiotherapy, which is why we focus treatment on achieving maximum function of your knee joint. It is important that the knee proprioception is good (position perception), and for all athletes, the return-to-sport phase of rehabilitation is crucial, during which we perform specific testing for specific sports and assess when the athlete is ready for full sports load after a meniscus injury.
In most meniscus injuries, improving muscle symmetry achieves greater stability of the damaged meniscus and more optimal kinematics of the knee joint. Using instrumental physiotherapy, we achieve an analgesic effect in case of pain. In the case of degenerative meniscus damage in the red zone, we perform therapy that accelerates healing.
Instrumental therapy is particularly important for meniscus injuries, as cartilage tissue regenerates very poorly on its own. The devices we use at MEDICOFIT clinic are: TECAR therapy, PERISO diamagnetic therapy, Summus LASER, and ultrasound therapy.
Physiotherapists will monitor your progress and constantly adapt the therapy to your abilities and needs.
Post-acute kinesiology
After the acute phase of treatment is completed, the kinesiology phase begins, which is aimed at restoring full load-bearing capacity and optimal function of your knee.
In this phase, we focus on special kinesiology training designed for improving knee joint stability and restoring full mobility that was impaired due to meniscus damage.
We usually make progress in strengthening the knee within a few weeks, allowing us to include more complex exercises in the therapeutic programme – this is especially important for athletes.
Once satisfactory progress is achieved, we begin to gradually introduce agility and plyometric exercises. These exercises facilitate a successful return to sports activities while reducing the risk of new injuries.
Kinesiology training contributes to increasing the patient’s awareness of correct movement techniques and knee loads in everyday life, which is crucial for preventing new injuries in the future.
All training takes place under expert supervision and is adapted to the individual capabilities of each individual. At the end of treatment, a knee test battery is also performed to assess the success of the treatment. This further increases the patient’s confidence in putting loads on the knee.
Preventive kinesiotherapy
Preventive training after a meniscus injury plays a key role in reducing the risk of re-injury and maintaining long-term knee health, which is why we have developed a post-rehabilitation programme at MEDICOFIT clinic.
Preventive training helps strengthen the muscles around the knee joint, which increases joint stability and reduces load on the meniscus. This is crucial, as a stable joint reduces the risk of uncontrolled movements and injury.
The selected training improves knee mobility, which allows for better shock absorption and thus reduces wear on the meniscus, while also strengthening ligaments and muscles and improving posture, which in turn reduces the risk of unintentional imbalance during physical exertion.
Because we believe in a comprehensive treatment, we guide you at MEDICOFIT clinic through the entire meniscus injury rehabilitation to free movement without pain and restore full strength and mobility to your knee.
DANGERS AND PITFALLS OF DELAYED REHABILITATION
MEDICOFIT specialists
Without specialist rehabilitation, long-term imbalance and instability of the knee accelerates the wear of the articular cartilage.
Patients experience instability and knee buckling, which increases the risk of further injury and permanent damage.
Inflammation of the synovial membrane surrounding the joint occurs, leading to chronic pain.
Inadequate or delayed rehabilitation seriously jeopardises an individual’s long-term physical health and is the main culprit for unsuccessful results and permanent movement limitations.
What do patients need to know about meniscus surgery?
The first treatment of a meniscus should always be conservative in the form of physiotherapy and kinesiology. At MEDICOFIT clinic, we are surprised that many patients seek surgical treatment before any conservative treatment. Such a procedure usually results in quick recurrence of the meniscus injury, as methodical physiotherapy is necessary to ensure optimal muscle function that stabilises the knee joint.
Patients with meniscus injuries must undergo physiotherapy and kinesiology as the first choice of meniscus treatment, and in the case of indicated surgical treatment, physiotherapy and kinesiology in the form of preoperative preparation of the knee joint.
Patients must start physiotherapy early after surgery, and if they have to wait for an appointment through a prescription, they should start physiotherapy in a private clinic. The greatest regression or setback in rehabilitation is caused by prolonging the first acute phase of rehabilitation.
Rehabilitation of a meniscus injury lasts 12–15 weeks and includes progressive escalation of exercises until the patient is ready for full loads. Even if the patient is not involved in sports, the knee joint needs to be optimally strengthened.
The meniscus must be preserved at all costs for as long as possible, as knee wear and osteoarthritis are accelerated at the site of removal. Studies clearly show a proportional correlation between the amount of meniscus removed with meniscectomy and the likelihood of developing knee osteoarthrosis.
Meniscus injury exercises
Below, we also present some effective exercises that you can incorporate into your routine to reduce discomfort and regain flexibility and strength in your meniscus. Performing these exercises correctly will help you improve your quality of life and prevent further injuries.
Important notice
• The exercise can be performed in numerous modifications and different load regimens; proper execution will be prescribed by a MEDICOFIT physiotherapy specialist for knee pain rehabilitation as part of your comprehensive treatment. • If you have knee problems, please book an diagnostic therapy appointment before performing the exercise. The exercise may also be contraindicated. • Always do the exercise strictly according to the prescribed regimen and as demonstrated by the physiotherapy specialist for knee joint rehabilitation and disorders. • We recommend the exercise as part of guided, comprehensive specialist physiotherapy for knee rehabilitation. • If you perform the exercise independently without the supervision of a physiotherapy specialist, we are not responsible for potential symptomatic responses.
Exercise no. 1: Single-leg bench dips with isometric phase below + lateral elastic band
Exercise no. 2: Isometric bridge with shoulder support + alternating forward foot transfer
Exercise no. 3: Single-leg side squats to a knee angle of 120° + medial deviation of the base
Frequently asked questions
Does an injured meniscus heal on its own?
The blood supply to the meniscus is poor. Both meniscuses are well supplied with blood at birth, but later only the outer edge of the meniscus, which is called the red zone, remains supplied with blood. If the meniscus is damaged in the white zone, the meniscus will not heal. If the meniscus is damaged in the red zone, there is a potential for healing, but it depends on the correct implementation of physiotherapy and kinesiology.
What complications can a meniscus injury cause?
A torn meniscus can cause a feeling that the knee is giving way, difficulty moving the knee, and persistent knee pain. If you do not undergo proper rehabilitation, there is a greater likelihood of developing osteoarthrosis in the injured knee.
Can I walk after a meniscus injury?
Yes, you can still walk with a torn meniscus. Simple walking and other activities that do not require turning, rapid changes of direction, and similar are usually well tolerated by patients. A meniscus tear can worsen over time, but the rate of progression is usually gradual and highly variable. Pain is always the guide – if the injury worsens, more severe pain usually occurs.
How are meniscus injuries treated?
Treatment for a meniscus injury may vary depending on the individual and the type of injury. Non-surgical approaches, such as the use of anti-inflammatory medications and rehabilitation with physical therapy, can help with most tears. Patients with more severe tears may need surgery – and treatment may also be adjusted depending on whether the injury is traumatic or degenerative.
When is meniscus surgical necessary?
Surgery is necessary in cases where the torn part of the meniscus is displaced, causing the knee to lock, and if the tear is associated with knee instability. We try to avoid surgery (if possible) using physiotherapy treatment, as any knee procedure increases the risk of knee wear and additional surgery.
Is physiotherapy necessary before meniscus surgery?
In the case of meniscus surgery, we recommend preoperative preparation in the form of targeted training to build muscle strength reserves, thereby preventing muscle atrophy after surgery, and in the form of neurostimulation training to maintain the maximum level of muscle activation. At MEDICOFIT clinic, preoperative preparation for a meniscus injury is usually performed within a time window of 8–12 weeks.
Book an appointment for meniscus rehabilitation
Viri in literatura
Beaufils, P., & Pujol, N. (2017). Management of traumatic meniscal tear and degenerative meniscal lesions. Save the meniscus. Orthopaedics & traumatology, surgery & research : OTSR, 103(8S), S237–S244. https://doi.org/10.1016/j.otsr.2017.08.003
Kopf, S., Beaufils, P., Hirschmann, M. T., Rotigliano, N., Ollivier, M., Pereira, H., Verdonk, R., Darabos, N., Ntagiopoulos, P., Dejour, D., Seil, R., & Becker, R. (2020). Management of traumatic meniscus tears: the 2019 ESSKA meniscus consensus. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA, 28(4), 1177–1194. https://doi.org/10.1007/s00167-020-05847-3
Twomey-Kozak, J., & Jayasuriya, C. T. (2020). Meniscus Repair and Regeneration: A Systematic Review from a Basic and Translational Science Perspective. Clinics in sports medicine, 39(1), 125–163. https://doi.org/10.1016/j.csm.2019.08.003
Brindle, T., Nyland, J., & Johnson, D. L. (2001). The meniscus: review of basic principles with application to surgery and rehabilitation. Journal of athletic training, 36(2), 160.
Sherman, S. L., DiPaolo, Z. J., Ray, T. E., Sachs, B. M., & Oladeji, L. O. (2020). Meniscus injuries: a review of rehabilitation and return to play. Clinics in sports medicine, 39(1), 165-183.
Luvsannyam, E., Jain, M. S., Leitao, A. R., Maikawa, N., & Leitao, A. E. (2022). Meniscus Tear: Pathology, Incidence, and Management. Cureus, 14(5), e25121. https://doi.org/10.7759/cureus.25121
This website uses cookies so that we can provide you with the best user experience possible. Cookie information is stored in your browser and performs functions such as recognising you when you return to our website and helping our team to understand which sections of the website you find most interesting and useful.
Strictly Necessary Cookies
Strictly Necessary Cookie should be enabled at all times so that we can save your preferences for cookie settings.
3rd Party Cookies
This website uses Google Analytics to collect anonymous information such as the number of visitors to the site, and the most popular pages. Keeping this cookie enabled helps us to improve our website.
Please enable Strictly Necessary Cookies first so that we can save your preferences!
Additional Cookies
This website uses the following additional cookies:
(List the cookies that you are using on the website here.)
Please enable Strictly Necessary Cookies first so that we can save your preferences!