Hip pain is a common and serious health problem that affects people of all ages. They can occur due to a variety of causes, including arthritis, bursitis, tendinitis, injury, or degenerative changes due to ageing. Regardless of the origin of the pain, it can significantly affect an individual’s quality of life, limit movement, and cause constant discomfort.
Inadequate or delayed rehabilitation seriously jeopardises an individual’s long-term physical health and is the main culprit for unsuccessful results and permanent movement limitations.
The dangers and pitfalls of neglecting physiotherapy treatment are serious. Without proper treatment, initially innocuous pain progresses and causes chronic problems such as permanent limitation of mobility, joint deformities, and an increased risk of surgery.
Physiotherapy treatment is crucial in managing hip pain, as it not only relieves unpleasant symptoms, but also addresses the underlying causes of your problems. With properly targeted therapy, we can improve mobility, strengthen the muscles around the joint, and reduce inflammation, which contributes to long-term improvement of the hip joint function.
Correct and timely physiotherapy treatment is crucial in restoring flexibility, strength, and freedom of movement.
The hip joint is designed to bear loads and provide mobility of the lower extremities. It has three functions:
allows mobility of the lower extremities,
transfers loads between the upper body, trunk and lower extremities, and
provides stable support during activities that involve bearing one’s own weight.
The hip joint is designed to ensure smooth performance of the functions described above. The pelvis is made up of three bones, which meet at an indentation on the outside. This is the socket for the head of the femur; together they form the hip joint. The hip joint is a ball-and-socket joint, which allows for a fairly high degree of mobility in all planes.
To perform a movement, a complex system of passive and dynamic stabilisers is required. Due to its great mobility, a large number of muscles pass over the hip joint, ensuring movement and at the same time ensuring the stability of the joint. The hip muscles originate from the pelvis and lumbar spine, and attach to the femur and also calf muscles.
During everyday activities, the hip joint is always under some load. To limit pain or possible wear and tear on the joint, it is necessary to reduce the impact of the reaction force on the joint, which means, among other things, reducing body weight (if necessary) and developing intermuscular coordination, thereby achieving coordinated functioning of the neuromuscular system and consequently a more balanced load on the joint. This can be achieved with the help of physiotherapy and kinesiology.
However, sometimes hip pain is caused by malformed bones or so much wear and tear over time that surgery cannot be avoided. Even in these cases, physiotherapy and kinesiotherapy in rehabilitation will successfully help restore function and ensure a life with less pain.
WHEN TO OPT FOR MEDICOFIT DIAGNOSTIC THERAPY?
If hip pain and any swelling do not subside within a week after an injury or without an obvious cause, it is necessary to undergo diagnostic therapy.
If hip pain is affecting your ability to walk, a diagnostic evaluation is necessary.
If you have previously had problems with your hip and the symptoms are recurring, this means that the injury was not properly treated or that a new injury has occurred.
At MEDICOFIT clinic, we provide patients with hip pain with scientifically supported specialist physiotherapy, which begins with booking a diagnostic therapy appointment.
Arthritis is a term for inflammation of the joints and surrounding structures. There are many different types of arthritis, the most common being osteoarthritis and rheumatoid arthritis, while rheumatic diseases also include gout and fibromyalgia. Osteoarthritis (OA) of the hip is a very common problem in Western society. It affects up to 25% of the population over the age of 55, affecting women more often than men, and genetic factors and lifestyle also contribute to its development with ageing.
Osteoarthritis is a progressive wear and tear of cartilage, resulting in bone rubbing against bone, which causes changes in the skeletal system. Of course, one change causes another, thus affecting also the soft tissue structures of the hip joint.
Hip pain that accompanies osteoarthritis occurs gradually. It may radiate forward into the groin or backward toward the buttock, thigh, or knee. Hip pain at night or pain at rest after activity is particularly characteristic. Joint stiffness in the morning or after prolonged rest is also characteristic.
When patients perform active hip flexion, they feel pain on the outside of the hip. Symptoms that accompany hip pain include the presence of snapping, grinding, skipping in the hip joint, limping, decreased joint mobility, and increased sensitivity. At the start of the disease, the greatest limitation occurs in the movement of abduction and rotation, but as the disease progresses, movements in other directions also become limited.
Osteoarthritis is a degenerative condition that will, without appropriate physiotherapy rehabilitation, progressively worsen and cause increasingly severe pain and movement restrictions.
Hip dysplasia
Hip dysplasia is a condition that includes various abnormalities in the anatomical shape of the femoral head and the joint socket – acetabulum, with which the femur is in contact. Due to the suboptimal shape of the bones, chronic changes occur over time, which are reflected in changes to the skeletal system as well as changes to the joint capsule, ligaments, and hip muscles.
Developmental dysplasia of the hip is common, and it is also the most common abnormality in the development of the locomotor system. Most (60–80%) abnormalities resolve spontaneously within eight weeks after birth.Hip dysplasia is also seen among the adult population. Some of them report problems since childhood, but most adults are unaware of the problem until they experience hip pain.
Hip pain usually occurs on the lateral side of the hip or in the front of the groin. It feels deep, as a result of chronic damage to the cartilage, labrum, or soft tissues on the side or front of the hip. It usually increases during activity and decreases with rest.
Hip pain can also occur due to excessive muscle tension. Specifically, the muscles that move the extremity connected to the hip away from the middle plane (abductors) must work more intensively because the acetabulum in hip dysplasia is shallower and does not provide sufficient support for the femoral head. The hip flexors also need to be more active, and sometimes hip pain is accompanied by a feeling of tightness, snapping, and skipping during activity. Hip pain at night occurs in about half of cases of hip dysplasia. If you experience such pain, seek professional help from a physiotherapy specialist.
It takes an average of about five years for adults with hip dysplasia to get a correct diagnosis, during which time they visit at least three different medical specialists. Therefore, if your problems persist, if hip pain occurs regularly and does not improve, seek a second opinion as soon as possible, as undiagnosed hip dysplasia can lead to early onset of degenerative changes.
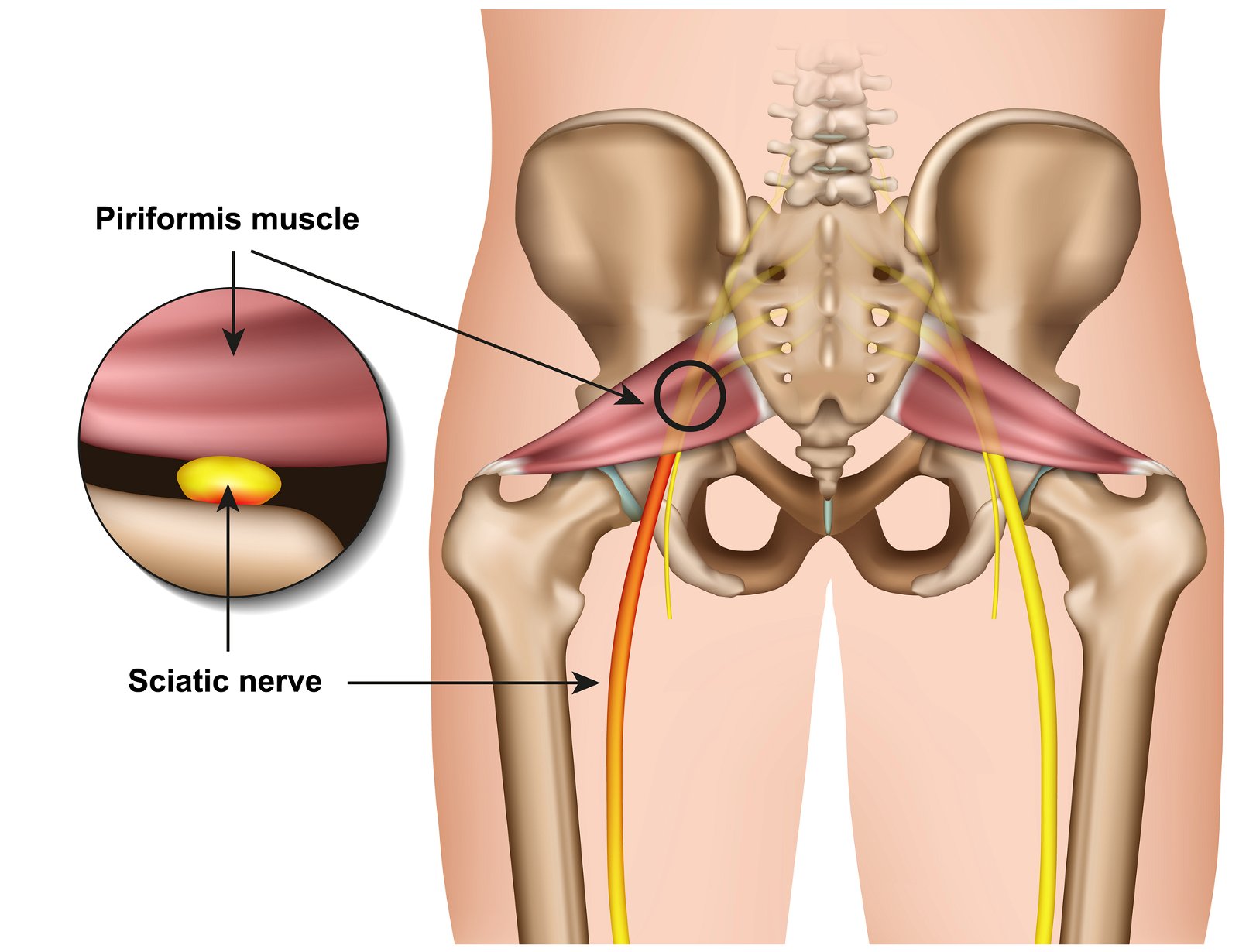
Piriformis syndrome
Piriformis syndrome is a neuromuscular disorder that occurs when the piriformis muscle compresses the sciatic nerve. The piriformis muscle is important in lower body movement, as it stabilises the hip joint and is responsible for lifting and rotating the thigh. The sciatic nerve runs along or through the piriformis muscle, down the back of the leg, and ends in the foot. A contraction of the piriformis muscle can cause nerve compression, leading to piriformis syndrome.
Hip pain from piriformis syndrome occurs in the buttocks and lateral hip area, and can occasionally be felt in the front of the thigh. The pain increases during activity, when getting out of bed, or when sitting for prolonged periods. It can be triggered by a specific movement that causes the pain to spread along the sciatic nerve down the leg.
Individuals report tingling, sharp pain that spreads down the leg, and numbness in the buttocks. The pain can be very severe. Often times piriformis syndrome is mistaken for sciatica, which includes pathology of the lumbar spine discs, causing compression of a nerve in the area where it exits the spinal canal.
Piriformis syndrome is unfortunately still too often misdiagnosed, so it is important to visit a hip physiotherapy specialist when pain occurs.
Hip impingement syndrome is also known by the abbreviation FAI (femoroacetabular impingement). Similar to hip dysplasia, impingement syndrome involves non-optimally formed articular surfaces of the acetabulum or the femoral head. In FAI syndrome, there are three morphological variations in the shape of the joint surfaces.
In the first type, called cam impingement, the head of the femur at the section where it meets the neck of the femur is not completely round, therefore making smooth movement impossible.When moving, it “hits” the cartilage inside the acetabulum and damages it, causing hip pain. In the second type of FAI, called pincer impingement, the acetabulum bone is shaped in such a way that it extends beyond the edges of its normal shape – it over-encircles the femoral head, causing increased friction and internal damage.The third type, called combined impingement, is a combination of the first two.
Hip pain associated with impingement syndrome is present on the lateral side of the hip, groin, or radiates to the buttocks, lower back, and thigh.Pain usually occurs during movement and is usually accompanied by limited mobility, clicking, snapping and skipping in the joint, joint stiffness and reduced function.
Burning pain in the hip may be present due to excessive friction of bone against bone. In FAI, hip flexion with internal rotation is often the most limited. Therefore, problems occur, for example, when climbing or descending stairs, where greater hip flexion is required than when walking on flat ground.
Hip bursitis
Hip bursitis is a condition in which the bursa – small fluid-filled sacs that act as friction cushions between the bones and soft tissues in the hip – become inflammed. The most common form is trochanteric bursitis, which causes pain on the outside of the hip – often the pain worsens when patients lie down on the affected side of the body.
It is more common in women and the elderly, with risk factors including repetitive strain, hip injuries, spinal diseases, and leg length discrepancy.
Our patients most often report hip pain that spreads along the outer side of the thigh and typically worsens at night and with movement. The diagnosis of bursitis is based on a clinical examination, and treatment includes physiotherapy techniques that strengthen the muscles and improve hip mobility.
Greater trochanteric pain syndrome – GTPS
Greater trochanteric pain syndrome (GTPS) is an umbrella term that encompasses various pathologies from bursitis to tendinopathies. It can occur due to tendon overload, incomplete and insufficient tendon healing, tendon compression, which occurs due to asymmetrical functioning of the soft structures in the hip, prolonged static position of the hip in flexion (e.g. while sitting), muscle imbalance and thus overload of certain structures, snapping hip syndrome, or as a result of hip osteoarthritis or iliotibial band syndrome.
Hip pain in GTPS is typically present on the lateral side. The area is extremely sensitive to touch, and the pain may spread down the side of the thigh toward the knee or back toward the buttock.
The pain is described as stabbing and intense, and there may also be a burning pain in the hip, which increases with simultaneous hip flexion and external rotation – i.e. the movement of placing the ankle on the opposite knee.
Hip pain also worsens when lying on the affected side, and sometimes lying on the unaffected side is also problematic, as the painful leg falls slightly downward, causing compression.
Hip pain at night can also be caused by impingement syndrome. Hip pain also occurs during activity when the leg is put under load – walking on level ground or up stairs, running, sometimes just standing is enough to cause pain. The pain also worsens during prolonged sitting or by sitting with your legs crossed.
In the case of hip pain, it is necessary to thoroughly analyse the entire body – both in a static position and during movement. There can be many causes of hip pain, just as there are many different anatomical structures in the hip area.
During examining, we must not overlook the effects of neighbouring joints. Hip pain may be just a secondary consequence, with the cause lying in the knee joint, ankles, or feet. What is happening higher up above the hip joint – in the torso – is also important.
A description of the pain also helps physiotherapists make a diagnosis. During your examination, try to describe the hip pain to your physiotherapist in terms of intensity, duration, location, and quality.
Intensity of hip pain
The physiotherapist will want to know about the severity of hip pain and when it occurs. We usually rate pain from 0 to 10, with 0 meaning no pain and 10 being the worst pain imaginable. An important information is also what makes the pain worse and what relieves it.
If hip pain worsens during movement, when muscles are under tension, we can conclude there may be soft tissue damage. During movement, we also cause a compressive force on the joint, which can be painful if the joint surfaces (bones, cartilage) are damaged.
If hip pain occurs at night, the trigger may be your position while sleeping. In the case of bursitis, sleeping on the affected side may cause irritation and consequently night-time pain. Similarly for osteoarthritis or piriformis syndrome, prolonged position can cause hip pain at night. Tendinopathy can also be a cause of hip pain at night. Tendons are known to warm up during activity, causing the pain to subside. Pain occurs 24 hours after activity.
Duration of hip pain
Depending on the duration, we can clinically distinguish acute pain, which is present for less than three months, and chronic pain, which is present for longer than three months.From the information on how long hip pain has been present, we can determine whether it is an injury that occurred at a specific moment, such as fractures, muscle or tendon tears, or whether it is a degenerative condition that is gradually worsening, as is typical of osteoarthritis.
Location of hip pain
The cause of hip pain can lie in various structures. Another important piece of information is whether the pain is only present locally, in a specific spot, or whether it radiates to neighbouring areas. In the event of nerve damage, pain is typically felt along the entire course of the nerve. For example, if the sciatic nerve is pinched, we will feel the pain all the way down to the big toe. To further confirm the diagnosis, it is advisable to undergo diagnostic imaging depending on the pathology, after consultation with an expert.
Quality of hip pain
The quality of pain is also very important information, which means how we feel the pain: is it sharp, dull, deep, superficial, burning, etc.? This information will provide the physiotherapist with insight into which hip structure is injured.
Burning hip pain can be present for several different reasons. It could be bursitis, tendinitis, muscle or nerve damage. Burning hip pain is felt as a strong, sharp, stabbing pain and is often accompanied by inflammation. Burning hip pain is common in the diagnosis of bursitis, impingement syndrome, and osteoarthritis, where damage to the joint surfaces occurs due to increased friction.
Changes in joint surfaces also lead to changes and inflammation in tendons or muscles. Burning hip pain also accompanies conditions involving a compressed nerve. We often also feel tingling, altered sensation, or numbness.
WHY CHOOSE SPECIALIST PHYSIOTHERAPY TREATMENT?
We ensure high treatment success and long-term results.
Proven lower risk of hip surgery!
We offer state-of-the-art non-invasive treatment methods that provide optimal conditions for healing of injuries and deformations of the hip joint.
Comprehensive treatment of hip pain at MEDICOFIT clinic is recommended by numerous renowned orthopaedic surgery specialists.
Due to the complexity of the hip pain rehabilitation process, it is important who you entrust with your body.
Hip pain is a common accompanying symptom of various pathologies. Because the body is a complex and interconnected system, often one pathology leads to another, causing problems in several joint systems at the same time.
Hip dysplasia, for example, can lead to osteoarthritis, which is accompanied by tendinopathy. At the same time, the altered dynamics of the hip affect the knee and spine, and suddenly it is difficult to know how and where to start solving problems that have arisen over the years. Therefore, do not attempt rehabilitation on your own.
Description of treatment When you first visit our clinic, we will perform diagnostic therapy, which allows us to make an accurate diagnosis, and already includes acute pain treatment and anti-inflammatory treatment, so you receive the first therapy as part of your diagnostic examination. Treatment at MEDICOFIT clinic includes the use of state-of-the-art pain relief modalities, such as extracorporeal shockwaves, HiToP electrostimulation, TECAR therapy, SIXTUS ultrasound therapy, PERISO diamagnetic therapy, and SUMMUS laser – the choice of therapy depends on your specific condition.
Depending on your specific pathology, we prescribe an individualised treatment programme, which includes stretching, strengthening, and endurance exercises. The special exercises help improve range of motion, muscle strength, and flexibility of the thigh muscles, which is especially important for patients with limited mobility.
We also perform manual therapy, which represents various joint and soft tissue mobilisation techniques that help improve mobility and reduce pain in combination with kinesiotherapy.
It is extremely important who you entrust with your body with in the rehabilitation process or in preventive training programmes. Proper progression can only be implemented by a team of experts from multidisciplinary fields who cooperate with each other, complement each other, understand the mechanism of injury and the specifics of the sport or recreational activity that the injured person wants to return to. At MEDICOFIT clinic, hip pain treatment is part of a comprehensive treatment with specialised physiotherapy and kinesiology.
DANGERS AND PITFALLS OF DELAYED REHABILITATION
MEDICOFIT specialists
Untreated hip pain leads to overuse and damage to the tendons and muscles around the hip joint.
Chronic hip pain caused by damage to the cartilage or joint surfaces results in premature wear and tear of the joint.
Incorrect compensatory posture causes pathological strain on the spine and related problems such as sciatica or herniated disc.
Exercises for hip pain
Below, we also present some effective exercises that you can incorporate into your routine to reduce discomfort and regain flexibility and strength in your hips. Performing these exercises correctly will help you improve your quality of life and prevent further injuries.
Important notice
• The exercise can be performed in numerous modifications and different load regimens; proper execution will be prescribed by a MEDICOFIT physiotherapy specialist for hip pain rehabilitation as part of your comprehensive treatment. • If you have hip problems, please book an diagnostic therapy appointment before performing the exercise. The exercise may also be contraindicated. • Always do the exercise strictly according to the prescribed regimen and as demonstrated by the physiotherapy specialist for hip joint rehabilitation and disorders. • We recommend the exercise as part of guided, comprehensive specialist physiotherapy for hip rehabilitation. • If you perform the exercise independently without the supervision of a physiotherapy specialist, we are not responsible for potential symptomatic responses.
Exercise no. 1: Double-leg squats in high angles of knee flexion + emphasised abduction
Exercise no. 2: Alternating single-leg hip flexions and abductions
Exercise no. 3: Double-leg hip lift from the floor + isometric adduction
What can you do on your own?
You can do a lot yourself to keep your hip joints healthy:
Rest: Rest and avoid movements that cause pain until the inflammation and pain subside.
Stretching and strengthening exercises: Regularly do stretching and strengthening exercises to improve mobility and strengthen the muscles around the hip, as advised by your physiotherapist.
Correct posture: Ensure proper posture when sitting and walking.
Maintaining a healthy body weight: A healthy body weight reduces pressure on the hips, whereas every extra kilogram increases the risk of degenerative changes.
If you are experiencing pain for a long time, visit a physiotherapy specialist for professional treatment and a tailored treatment plan.
Book an appointment for hip pain treatment
References and literature
1.American Academy of Orthopaedic Surgeons. Diseases and conditions: Osteoarthritis of the hip.Available at: https://orthoinfo.aaos.org/en/diseases–conditions/osteoarthritis-of-the-hip [20.9.2022]
Brunker & Khan’s. Clinical sports medicine. Hip related pain. pp: 510-545.
Ganderton, C., Semciw, A., Cook, J., Moreira, E. & Pizzari, T.. 2018. Gluteal loading versus sham exercises to improve pain and dysfunction in postmenopausal women with greater trochanteric pain syndrome: a randomized controlled trial. Journal of Women’s Health. 1;27(6), 815-29.
Hlebš, S., Slakan Jakovljević, B. & Klauser, M., 2014. Manualna terapija – sklepna mobilizacija udov testiranje in terapija. Univerza v Ljubljani, Zdravsvtena fakulteta, pp 86-87.
International hip dyspalsia institute. Adult Diagnosis. Available at: https://hipdysplasia.org/adults/diagnosis/[20.9.2022].
International hip dyspalsia institute. If you have hip dysplasia, you are not alone. Avaliable at: https://hipdysplasia.org/adults/[20.9.2022].
Kodarin, Jan. 2017. Najpogostejše poškodbe kolčnega sklepa in gibalnoterapevtski pristopi k zdravljenju. Diplomsko delo. Koper: Univerza na Primorskem.
Lespasio MJ, Sultan AA, Piuzzi NS, Khlopas A, Husni ME, Muschler GF, Mont MA. Hip osteoarthritis: a primer. The Permanente Journal. 2018;22. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5760056/ (last accessed 19.11.2019)
Wahoff, M., 2014. Rehabilitation after labral repair and femoroacetabilar decompression: Criteria-based progression through the return to sport phase. The International Journal of Sports Physical Therapy, 9(6), pp 813
This website uses cookies so that we can provide you with the best user experience possible. Cookie information is stored in your browser and performs functions such as recognising you when you return to our website and helping our team to understand which sections of the website you find most interesting and useful.
Strictly Necessary Cookies
Strictly Necessary Cookie should be enabled at all times so that we can save your preferences for cookie settings.
3rd Party Cookies
This website uses Google Analytics to collect anonymous information such as the number of visitors to the site, and the most popular pages. Keeping this cookie enabled helps us to improve our website.
Please enable Strictly Necessary Cookies first so that we can save your preferences!
Additional Cookies
This website uses the following additional cookies:
(List the cookies that you are using on the website here.)
Please enable Strictly Necessary Cookies first so that we can save your preferences!