In this article we will talk about calcification, a common state where calcium deposits build up in undesired places. Our main focus is going to be the shoulder muscles commonly named the rotator cuff.
Calcium crystals are often deposited in the tendons of these muscles and/or the surrounding bursae. The state is typically accompanied by pain that worsens at night and limited mobility.
For a better understanding of this condition, we should first look at all the structures found under the skin and potential problems that can occur if something goes wrong.
Shoulder is comprehended as a multi-joint system
The word “shoulder” is generally understood as a side upper part of the trunk above the thorax where an arm begins (7). In anatomy this is defined as a shoulder joint that marks the juncture between the humerus and the scapula called the glenohumeral joint.
Accompanied by other nearby structures, a shoulder joint forms a shoulder girdle. The shoulder girdle consists of humerus, scapula, clavicle and sternum. It is a complex system which requires normal function of all the mentioned structures as well as the spine for perfect operation.
In order to move the skeleton, soft tissue that attaches to it is required. We know two types of this tissue called static and dynamic stabilizers. Static stabilizers consist of bone and cartilaginous structures, intra-articular pressure and ligaments. Dynamic stabilizers are rotator cuff muscles and other muscles of the shoulder girdle.
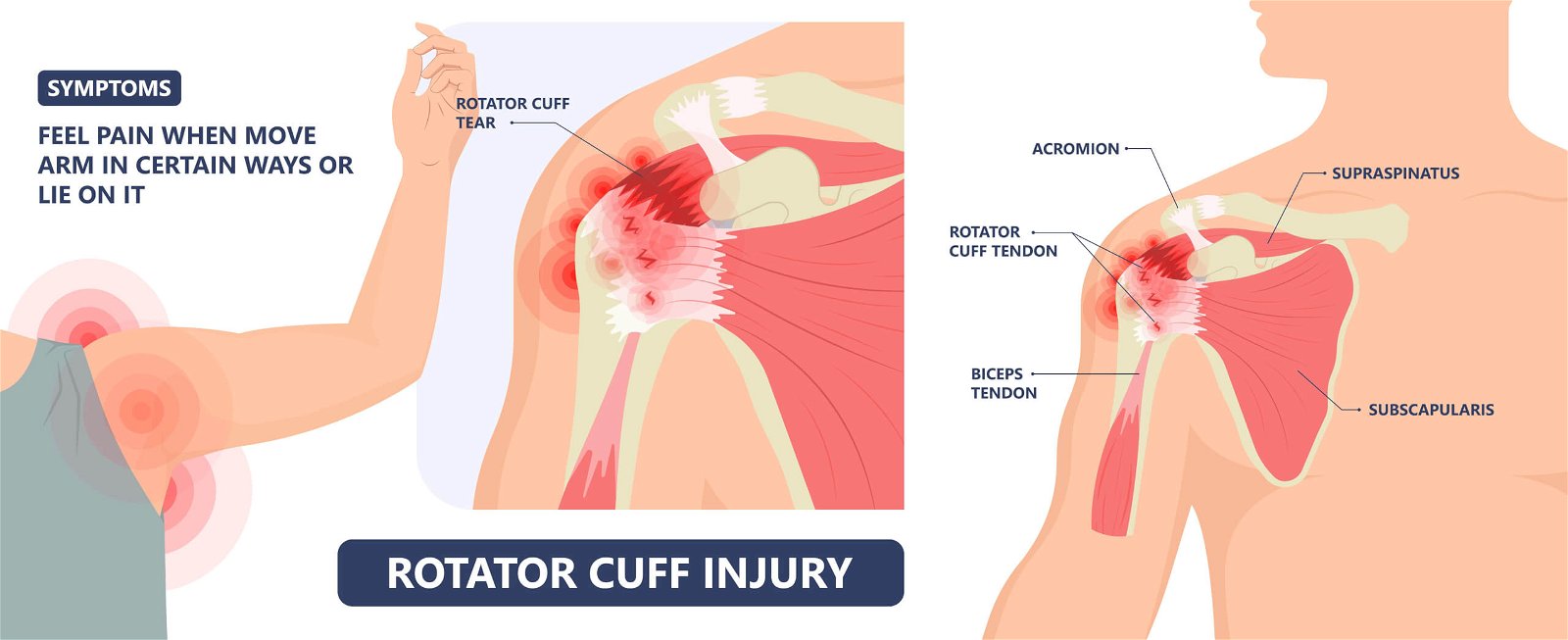
Therefore rotator cuff is a common name for four muscles that move the glenohumeral joint and provide its stability. These muscles are m. supraspinatus, m.infraspinatus, m. subscapularis in m. teres minor. The muscle supraspinatus abducts the arm at the shoulder joint. Furthermore, m. subscapularis performs internal rotation. Lastly, m. infraspinatus and m.teres are external rotators of the shoulder.
All these muscles insert into the head of the humerus and are tightly fastened inside the capsule of the shoulder joint. Together they form a cuff, hence the name rotator cuff (4).
The shoulder girdle is outstanding because of its flexibility, which requires soft tissue to be elastic and stretchable while providing consistent stabilization.
It is also important to mention the bursae, which are like pillows that reside between muscle tissue or tendons and other tissue to reduce friction and enable smoother gliding of a tendon or a muscle during movement.
What does calcification of the shoulder even mean?
The more accurate technical term would be calcification tendinitis of the rotator cuff, which more precisely defines that the changes occur in one of the tendons of rotator cuff muscles. A tendon is a type of connective tissue.
How often does calcification tendinitis of the rotator cuff occur?
According to X-ray, calcification tendinitis of the rotator cuff occurs in 2,7 to 10,3% of the adult population with approximately 50% becoming symptomatic over time (6). Women seem to be more prone to it, while 70% of all the patients are female, mostly aged between 30 and 60 (5).
Statistically speaking, the tendon of muscle supraspinatus seems to be the most affected (80%), followed by the tendon of m. infraspinatus (15%) and the tendon of m. subscapularis (5%)(1).
Causes of shoulder calcification
Why this state even arises and why some experience pain and others do not remains unclear. With evidence we are familiar with we can briefly say that numerous factors regarding one’s body such as gender, aging, specific metabolic or cellular state and recurrent mechanical strain result in an environment where tissue begins to alter and calcium crystals are deposited in tendons.
This means that to a certain extent the formation is influenced by factors that cannot be affected and those are the aforementioned female sex and age. Various metabolic, autoimmune, and rheumatic diseases, such as diabetes, rheumatoid arthritis, or the decreased activity of the thyroid gland, are also contributing factors.
At the same time, the formation of calcific tendinopathy is also caused by the individual’s environment and their work. Those who are at most risk are the individuals who oftentimes use an extended arm position with internal rotation and slight abduction – such are for example office workers, cashiers, tailors, hairdressers, production line workers, dentists, etc. (6).
If you desire a more detailed explanation of the formation theory, read the paragraph below where you will have to make it through some technical terms.
One of the possible theories of the pathology is that when the arm is kept in the mentioned position for a long time, the muscles that contract create hypoxic conditions (the concentration of oxygen decreases), which causes a fibrocartilaginous change in the tissues, followed by the deposition of calcium deposits.
Another possible theory is the conversion of tenocytes to chondrocytes, causing tendon calcification. A third theory, however, assumes that the process is the result of incorrect differentiation of stem cells in the tendon into bone cells (1, 3).
Phases of development
In any case, the process is most likely a combination of multiple factors and is split into three phases according to the stages of the development of the condition:
Pre-calcific phase: The individual does not notice any symptoms, nor are they identifiable via diagnostic imaging. What is happening is that the number of tendon cells is being reduced and the number of bone cells is increasing.
Calcific phase: First begins the build-up of calcium deposits in the tendon, which can only be observed by X-ray imaging or ultrasound. Then the resorptive phase starts, characterized by pain that persists even during periods of rest and sometimes does not respond to conventional analgesics. It is a period of ongoing processes where the body wishes to reabsorb the calcium crystals and eliminate them which leads to an inflammatory reaction and an increase in pressure inside the tendon. Swelling may also be present.
Post-calcific phase: It is a period of remodelling and self-treatment of the tendon, which can last for several months.
When to seek professional help
The natural cycle that is otherwise oriented towards self-healing of the tendon can be disrupted by various causes. Relatively poor circulation at the tissue site and the rather difficult biomechanical conditions can be the reason for the failure to fully heal (6).
With modern methods of diagnosis and rehabilitation, it is sensible to seek professional help as soon as possible when problems occur, because we know how to successfully relieve your symptoms. If rotator cuff calcific tendonitis is suspected, your doctor will refer you for an X-ray, which will verify the presence of calcium crystals.
Ultrasound diagnostics is also possible, which enables the assessment of soft tissues – what is the integrity of the rotator cuff and what is happening with the bursa. A quality clinical examination is also important, where a specialist doctor or a physiotherapist assesses the impairment of individual structures using various manual tests.
Quality diagnostics is of utmost importance for further treatment, because only in this way will the rehabilitation be properly directed and managed, and you will not waste your precious time and days of pain wandering in the dark.
The treatment of the calcification is usually conservative
The first choice of treatment is non-surgical. It includes physiotherapeutic treatment and pain relief with analgesic therapy. Early participation in physiotherapy can prevent your condition from worsening and escalating into shoulder girdle stiffness or into a “frozen shoulder” state (1).
Therapy includes pain-relieving procedures and methods for accelerating and promoting the healing of the tissue, exercises and techniques for maintaining and gaining mobility, and procedures that aim the reduction swelling and preserve or gain muscle strength.
If the condition does not change after six months of physiotherapy and the symptoms persist, it is necessary to consider surgery. This usually does not happen as we are successful with physiotherapeutic techniques (3, 6).
Extracorporeal shock wave therapy
One of the most common and successful physiotherapeutic interventions when treating rotator cuff calcific tendonitis is extracorporeal shock wave therapy.
Extracorporeal shock wave therapy is a non-invasive procedure, where a »loud« device uses a probe to transmit high-energy waves into the tissue. A sudden mechanical compression produces a series of low-amplitude, high-frequency waves.
The repeating waves thus spread the energy deep into the tissue (2). The therapy is carried out with a frequency of 1 – 20 (Hz) vibrations per second and determines the comfort of the patient – the higher the frequency, the easier it is to tolerate the therapy.
The therapist will also determine the pressure, which depends on the area itself, the pain threshold of the individual, and successive therapies.
The number of individual pulses is also set, which are once again individually conditioned. Usually, around 2000 to 3000 pulses are administered to the affected area per therapy. Between individual sessions, a few-day break is necessary, and the number of therapy sessions is determined individually according to the condition.
How do extracorporeal shock waves contribute to the treatment of calcifications?
The effects of extracorporeal shock waves are based on pressure changes inside the tissue, which subsequently leads to an increase in the metabolic activity of cells and an increase in the local blood flow (2). This aids the regeneration of the tissue, stimulates and promotes the healing of the tissue, stimulates the growth process of new blood vessels, and affects the relaxation of muscles and resorption of calcium deposits.
Due to the pulses that are introduced to the tissue, pain nerve fibers are also stimulated, which inhibits the transmission of individual pain stimuli from the affected tissue, which is felt like a reduction in the level of pain (2, 3). Extracorporeal shock waves affect the calcium crystals in such a way that they cause the formation of microscopic bubbles and with that, they change the shape and size of calcium deposits. It could be said that they break down the crystals and facilitate their absorption post-therapy (2, 3).
The use of this procedure is prohibited in those who use anticoagulant therapy, in pregnant women, and in those with severe osteoporosis or possible malignant conditions (2). The procedure is not the most pleasant, it could even be said that it is painful, and as a side effect the occurrence of a hematoma is not unusual.
However, the therapy is effective and contributes to more successful treatment of rotator cuff calcification.
physiotherapy for calcification of the rotator cuff at the Medicofit clinic
Rotator cuff calcific tendonitis can be a very unpleasant and not so rare condition that causes pain, reduced mobility, and thus reduced functionality of the shoulder. We are all very well aware of how necessary normal shoulder function is when performing daily activities.
The downside of the diagnosis is that the course of the condition can be long, but the upside is that with modern approaches we know how to help you, ease the symptoms, and speed up the healing process. At Medicofit clinic, we have already successfully helped people with rotator cuff calcific tendonitis.
With the cooperation of the centre of physiotherapy and the centre of kinesiology, we offer you a holistic approach, in which we will focus on reducing pain and accelerating healing. We can effectively help you with this by using extracorporeal shock waves.
We will also implement various approaches and techniques for increasing mobility and gaining muscle strength with the desire to return to normal life activity as soon as possible.
References
Chianca, V., Albano, D., Messina, C., Midiri, F., Mauri, G., Aliprandi, A., Catapano, M., Pescatori, L. C., Monaco, C. G., Gitto, S., Pisani Mainini, A., Corazza, A., Rapisarda, S., Pozzi, G., Barile, A., Masciocchi, C., & Sconfienza, L. M., 2018. Rotator cuff calcific tendinopathy: from diagnosis to treatment. Acta bio-medica : Atenei Parmensis, 89(1-S), 186–196.
Ipavec, M., 2015. Kratek pregled uspešnosti zdravljenja patologij ramena z udarnimi globinskimi valovi. In: Rama v ortopediji. XI mariborsko srečanje. Maribor: Medicinska fakulteta, 137 – 141.
Kachewar, S. & Kulkarni, D.S., 2013. Calcific Tendinitis of the Rotator Cuff: A Review. J Clin Diagn Res, 7 (7), 1482-1485.
Milić, M., 2015. Kalcinirajoči tendinitis. In: Rama v ortopediji. XI mariborsko srečanje. Maribor: Medicinska fakulteta, 161 – 167.
Sansone, V., Consonni, O., Maiorano, E., Meroni, R., Goddi, A., 2016. Calcific tendinopathy of the rotator cuff: the correlation between pain and imaging features in symptomatic and asymptomatic female shoulders. Skeletal Radiol. 45(1):49-55
Sansone, V., Maiorano, E., Galluzzo, A., & Pascale, V., 2018. Calcific tendinopathy of the shoulder: clinical perspectives into the mechanisms, pathogenesis, and treatment. Orthopedic research and reviews, 10, 63–72.